
Medication- and Toxin-Induced Tinnitus (Ototoxicity)
I, too, was once affected by extreme tinnitus that turned my entire life into a living hell. In my case, the primary trigger back then was the classic noise-induced tinnitus (and not an acute medication event), but the constant sound was exactly the same permanent assault on my nerves, my sleep, and my entire life. Doctors often told me too that I just had to learn to live with it.
I'm writing this article about the chemical triggers because the topic played an important role in my own research. Since 2012, I've been intensively engaged with cellular biochemistry — including the field of toxicology and environmental medicine. And this is where it all comes together: with reputable environmental medicine practitioners (such as Dr. Klinghardt or Dr. Mutter), one frequently observes a fascinating phenomenon in practice. When tinnitus patients have a hidden toxin or heavy metal load as a contributing cause, a targeted, cellular detoxification approach is often reported to bring noticeable relief from the ear sounds. What I share here is my current understanding from this research — and the foundation for the approaches we'll cover later on this site, based on this research.
Important notice: Never stop prescription medications on your own! For ear sounds related to taking medication — especially if they came on suddenly — please consult a physician promptly to clarify the next steps. Any change to your medication needs to happen under medical supervision.
The Chemical Attack From Within
When we think of tinnitus, two images usually come to mind right away: the booming concert (noise), or massive stress and inner trauma stress (psychosomatics). But there's a third trigger that's neither mechanical nor emotional — it's purely chemical: medication- or toxin-induced tinnitus. In my view, this type of tinnitus is among the least common — but for the sake of completeness, I want to share my view on this third trigger as well. In technical terms, this is called ototoxicity (literally: „ear toxicity“).
It might sound abstract at first, but our inner ear is extremely sensitive to certain chemical substances. Some medications or environmental toxins can travel through the bloodstream directly into the inner ear, where they can irritate or even damage the sensitive hair cells or the auditory nerve.
The Mechanism: How Chemistry Generates Sounds
Recall the image of the „stuck piano key“ from the section on noise-induced tinnitus. In a noise trauma, mechanical force (sound waves) bends or damages the hair cell.
In medication- or toxin-induced tinnitus, something very similar often happens in the end — just through a different path. You essentially have to picture each individual hair cell in the ear as a small biological battery. It maintains an extremely fine balance of energy (ATP), minerals, and electrical voltage.
If this fine balance is now massively disturbed by chemical substances (environmental toxins or toxic medication doses), here's what happens at the cellular level, according to my understanding of the biochemistry:
The cell's energy level (ATP) drops. As a result, the tiny pumps in the cell wall simply can no longer keep up with maintaining the chemical balance. As a consequence, calcium accumulates inside the cell. Because calcium in biology is the direct trigger for stimulus transmission, this ion excess forces the cell to fire „false signals“ permanently and uncontrollably. For me, this isn't a mystical coincidence — it's a logical biochemical automatism. The brain perceives this electrical permanent firing as a sound.
Which exact tone you hear — whether a high whistling, a hissing, or a low rumbling — usually just depends on the exact location in the cochlea where the affected hair cells sit. The ear isn't usually physically destroyed in this moment — but its fine inner order falls out of rhythm.
The Electrical Short Circuits (The Auditory Nerve)
It's not only the hair cells that are in danger — the „power cable“ itself is too: the auditory nerve. This nerve is surrounded by a protective sheath, the myelin. This insulating layer is extremely rich in fats and minerals, and so it reacts particularly sensitively to toxins circulating in the blood. When this sheath is weakened or „thinned out“ by chemical stress, the nerve no longer transmits signals cleanly. Real electrical „short circuits“ develop.
And this is where the pure logic of our anatomy reveals itself: our auditory nerve isn't a simple single wire — it's a thick bundle of thousands of tiny nerve fibers. Each individual fiber is responsible for transmitting a particular tone pitch. When the toxic short circuit (the myelin breakdown) now occurs at exactly the nerve fiber responsible for high frequencies, your brain logically registers a high whistling. If a fiber for low tones is affected, you hear a low rumbling. So whichever hissing, whistling, or sound you perceive is absolutely no coincidence — it depends decisively on which tiny spot in the main cable the insulation got damaged.
The Universal Law of Tinnitus
When you put all these puzzle pieces together, a central common denominator crystallizes: in my deepest conviction and experience, tinnitus is ultimately the result of chronically irritated, overstimulated hearing-processing nerves. Physically, it almost doesn't matter where exactly the starting shot for this overstimulation goes off:
- Whether the hair cells (through noise or medications) are stuck in emergency mode and permanently flood the auditory nerve with glutamate…
- Or whether environmental toxins and heavy metals attack the insulation (myelin) of the nerves and cause direct short circuits there…
- Or whether massive, chronic psychosomatic stress builds up in the brain and puts the hearing-processing centers under permanent current „from above“…
Once you've understood this universal logic, the tinnitus often loses much of its mystical horror.
The end result, in my experience, is almost always exactly the same: the nervous system in this area is chronically irritated and broadcasts an electrical SOS permanent firing. Once you've understood this universal logic, the tinnitus often loses much of its mystical horror — and a possible path forward becomes much clearer.
Typical Triggers (Ototoxic Substances)
But okay, let's get into it: there's a whole range of substances that are known to potentially have ototoxic effects. (Important: this isn't a medical list for self-diagnosis — it just serves general understanding!)
1. Medications
Some preparations can overstimulate the inner ear. But it's not enough to just know their names — you have to understand why they throw the system off track. Only when we grasp the mechanics of the damage does our later approach (cellular energy and detoxification) make any sense at all. Among the best-known groups are:
(As stated in the important notice above: any change to your medication needs to happen under medical supervision.)
High-dose pain medications (especially aspirin/ASA)
First, some reassurance: a normal headache pill usually doesn't cause tinnitus. According to research, there's often a strict dose paradox here. It usually only becomes dangerous at real toxic high doses (often several grams a day). When that happens, pharmacological models suggest that the medication triggers a three-stage chain reaction in the inner ear:
- The motor stutters: The assumption is that the active substance blocks prestin, a tiny protein that works like a motor in the outer hair cells. As a result, the acoustic amplifier in the ear collapses. As a panic reaction, the brain often turns its central „volume knob“ (Central Gain) up to maximum, just to hear anything at all.
- Nerve over-sensitivity: At the same time, models suggest that the medication puts the receptors at the auditory nerve into a state of elevated excitability. The stimulus threshold drops, which means the nervous system already reacts much more sensitively to the smallest signals.
- The power outage (the ignition): According to biochemical research, aspirin in high doses works as an „uncoupler“ in the mitochondria. Metaphorically speaking, it pulls the cell's power plug (ATP deficit). And here's the fascinating, logical difference compared to noise trauma: with noise, mechanical force literally bends the fine hairs of the cell. As a result, the calcium channel stays permanently open like a stuck door, and calcium streams in unchecked. With aspirin overdose, that doesn't happen. The hairs stand completely intact, in place. Here, it's „just“ the chemistry that's fallen out of balance. No more calcium streams in than usual — but because of the rapid energy drop, the cell's tiny calcium pumps simply can't keep up with pumping it back out. In that moment, the cell is simply completely overwhelmed by the normal calcium influx. The end result is the same: calcium accumulates inside and forces the cell to release the neurotransmitter glutamate non-stop.
The possible tinnitus result: this uncontrolled glutamate flood hits nerves with an already-lowered stimulus threshold (Stage 2) and gets sent to a brain whose volume knob is at the limit (Stage 1). A deafening permanent firing develops. And this exact simple cellular logic also explains an everyday phenomenon for which a clear answer isn't always immediately available. To take a fictional example: why does the uncle who heavily overdosed on aspirin for a week often have his ears quiet down again shortly after stopping — while the 26-year-old nephew, who only went to two loud clubs, has been suffering for four months from a tinnitus that just won't go away? For me, the answer is crystal clear: in the uncle's case, it was a biochemical power outage. Once the medication is stopped under medical guidance and flushed out of the bloodstream, the cell's power plants can fire up again, the pumps clear away the calcium, and the system can work without errors again. In the nephew's case, however, there was raw mechanical force at play. His fine hairs are physically bent or stuck together. That's like having the hinge of a door bent by brute force — logically, that doesn't just repair itself over a weekend, just because the noise is over.
Certain antibiotics (aminoglycosides)
These powerful antibiotics are mostly only used in hospital settings for severe bacterial infections (e.g., gentamicin). They have an extremely tricky property: they often selectively accumulate in the fluid of the inner ear and only get broken down from there excruciatingly slowly — they can remain there for weeks or months. There, they react with iron in the body and generate a massive explosion of „free radicals“ (ROS). It's like a biochemical wildfire that attacks the sensitive cell membranes and the inner actin scaffolding of the hairs. Here's where a simple biological logic with two outcomes applies:
- Outcome 1 (cell death): If the body is already weakened at this point, has hardly any nutrient resources, or has pre-existing damage, the cell completely collapses under this chemical wildfire and dies (apoptosis). The paradoxical result: in this case, no tinnitus usually develops. A dead cell no longer broadcasts. Instead, a pure, silent hearing loss (deafness) develops in exactly that frequency.
- Outcome 2 (the survival struggle = the tinnitus): The cell barely survives the attack but remains massively structurally damaged. It's basically exactly like a noise trauma — just chemically triggered. The rigid inner skeleton (actin) collapses, which causes the hairs to literally wilt like flowers without water. But the cell still lives! And because it lives, it desperately tries to fight against the calcium streaming in through the leaky membrane. Because this ion influx is the direct chemical command for stimulus transmission, the heavily damaged cell is forced, in permanent panic mode, to fire the neurotransmitter glutamate non-stop to the auditory nerve. This cellular survival struggle becomes an electrical permanent firing — and that's exactly what you perceive as tinnitus.
Diuretics (strong-acting water pills)
So-called loop diuretics not only remove water from the body, but also massively flush out electrolytes like potassium and sodium. The problem? The inner ear has its own small voltage source, the stria vascularis. This tissue layer constantly pumps potassium into the ear fluid to maintain a constant electrical voltage there — that's the battery the hair cells draw their current from for hearing. Water pills block exactly this biochemical pump mechanism. As a result, the electrical voltage in the ear crashes massively. The biological battery is suddenly „empty,“ and the hearing system enters a chaotic alarm state, which discharges as hissing or whistling.
Chemotherapeutics (such as cisplatin)
These aggressive cancer medications are often based on platinum (a heavy metal). They're programmed to interfere with the DNA of cells. When this medication does cause a tinnitus event, according to pharmacological models, it's due to a real biochemical wildfire in the inner ear: in this case, cisplatin completely robs the cell of its most important built-in protective substance (glutathione). Without this protective shield, free radicals eat microscopic holes into the cell membrane and destroy the ion pumps. The result is an extreme ion imbalance: calcium floods the cell and forces it into permanent glutamate firing. At the same time, cisplatin is strongly neurotoxic and literally breaks down the myelin sheath (the insulation) of the auditory nerve. When the permanent firing of the damaged cell now hits an unprotected, exposed nerve, real measurable short circuits and misfires arise directly on the main cable to the brain. And here too, the biological tinnitus fork applies: if the cell is completely destroyed (apoptosis), silence (deafness) usually develops. If it survives as a heavily damaged ruin with leaking membranes and exposed nerves, it often fires a permanent disturbance signal. That explains why chemo-tinnitus is often extremely persistent.
Quinine (malaria medications & anti-muscle-cramp preparations)
Quinine has a strongly vasoconstrictive effect. The inner ear is an absolute anatomical dead end — it's supplied with blood by only a single tiny artery (arteria labyrinthi). There are no „detours“ there. When quinine now narrows this tiny artery, and at the same time makes the red blood cells less flexible, the blood flow gets stuck. The hair cells are then cut off from the oxygen and nutrient supply they absolutely need. They go into massive oxygen deprivation and immediately switch into tinnitus panic mode.
2. Heavy Metals and Environmental Toxins
Heavy metals like mercury, lead, aluminum, or cadmium act on the cellular level like extremely aggressive saboteurs. Anyone who works with deep detoxification protocols knows: they don't just diffusely poison the cells of the inner ear — they latch onto biological processes specifically and block them. This happens in the cochlea and at the auditory nerve through four extremely destructive mechanisms:
- 01Trojan Horse
- 02Thiol Hack
- 03Wrecking Ball
- 04Myelin Shredder
Mechanism 1: The Trojan Horse (Trace Element Displacement)
Metals like cadmium, mercury, etc. often have a striking chemical similarity to vital trace elements — especially zinc and selenium. The body gets fooled and incorporates the heavy metal into proteins in place of the zinc. The result is fatal: at the auditory nerve receptors, zinc functions as a kind of natural „brake.“ It ensures that the nerve doesn't immediately overreact to every tiny stimulus. When a heavy metal displaces this zinc, this brake completely fails. The acoustic signals slam unchecked into the nervous system, which in my experience shows up as a deafening tinnitus. At the same time, the displacement of selenium massively disrupts the production of the body's most important antioxidant (glutathione). Cell protection threatens to collapse.
Mechanism 2: The Thiol Hack (The Bending of the Proteins)
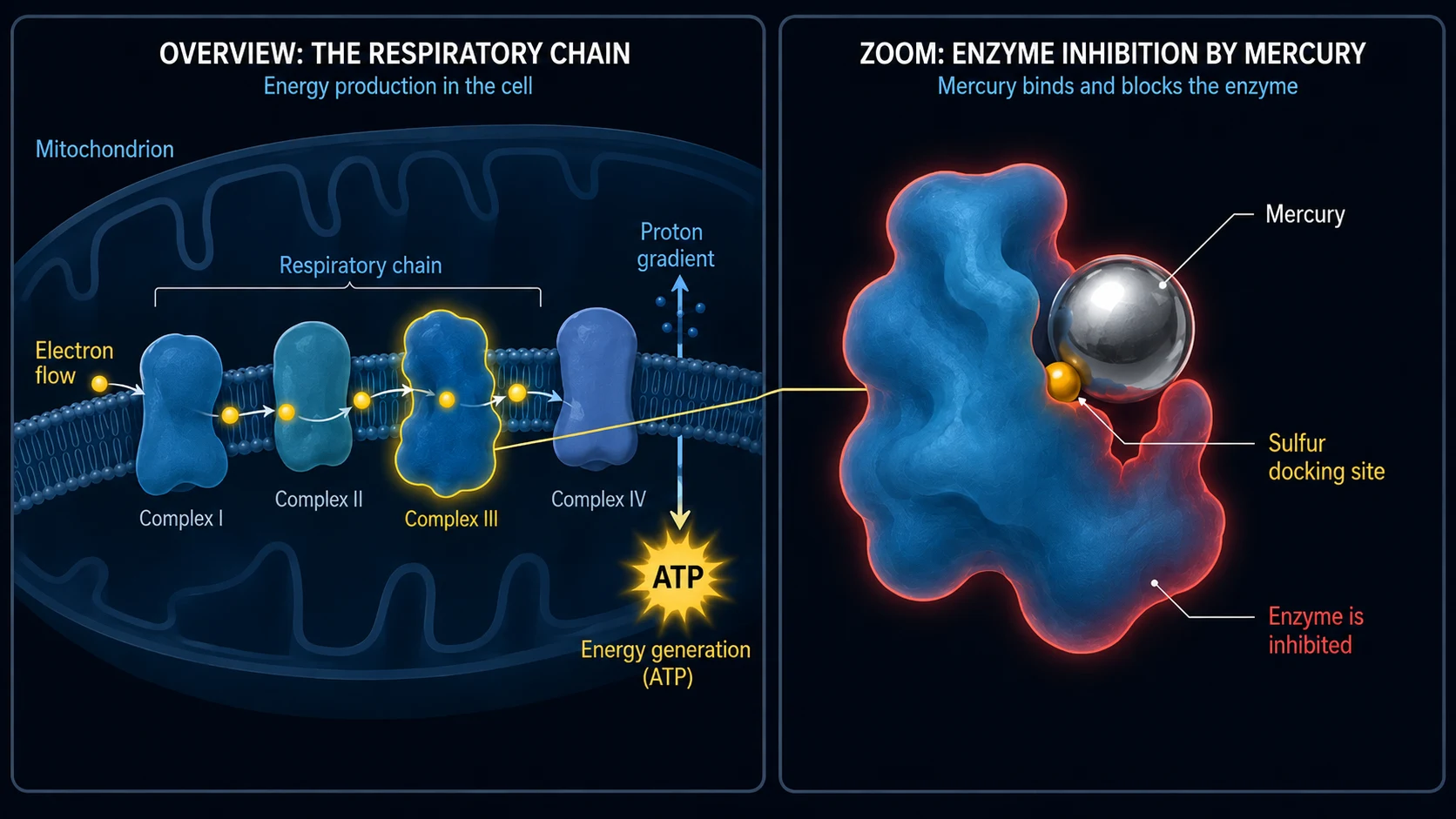
Heavy metals also have an enormous chemical preference for sulfur. Most of our enzymes and tiny cell pumps (such as the ATP-driven calcium pumps) have sulfur-containing docking sites, called thiol groups (-SH). When the heavy metal arrives in the inner ear, it immediately docks onto these sulfur groups. The moment the metal connects with the enzyme, it forces the protein to change its 3D structure — it literally bends. As a result, the calcium pump of the hair cell gets blocked and falls out of function.
Mechanism 3: The Biological Wrecking Ball (Direct Cell Destruction)
Besides sabotaging pumps, metals also attack the cell's hardware directly and physically. Lead and cadmium penetrate into the mitochondria (the cell's power plants), settle into the cellular respiratory chain, and massively choke off ATP production. Metaphorically speaking, the cell threatens to suffocate from within. At the same time, the metals in the ear trigger an explosion of free radicals that literally oxidize the fat-rich protective sheath (membrane) of the hair cell — it goes rancid, melts, and becomes leaky (lipid peroxidation). Toxic calcium streams in like through a broken dam. On top of that, the metals attack the rigid protein scaffolding (actin) inside the tiny sensory hairs. The molecular bridges break, the hairs wither, kink off, and lock the stimulus channels in a permanently open position.
Mechanism 4: The Myelin Shredder (Attack on the Main Cable)
Heavy metals also eat their way directly into the cable itself — the auditory nerve — and destroy its insulating layer, the myelin. This layer is almost 80% fats, which makes it the perfect victim for oxidative stress. The free radicals literally etch the fat away. Mercury, for example, binds to the „myelin basic protein,“ the molecular glue of the insulating layer, which causes it to flake off. In toxicology, lead is strongly suspected of going one step further and specifically damaging the so-called Schwann cells — the tiny construction workers responsible for repairing the myelin. Without insulation, the electrical signals of hearing slow down massively, jump over to neighboring exposed nerve fibers (cross-talk), and generate massive misfires.
-
01Chemical entry
A medication in toxic high doses, or a heavy metal / environmental toxin, reaches the inner ear via the bloodstream.
-
02Balance tips
ATP drops, the pumps can't keep up, calcium accumulates inside the cell, the myelin thins out.
-
03Permanent faulty signal
The weakened cell fires glutamate non-stop, or signals jump over to neighboring fibers — the brain perceives it as a tone.
But Then Why Doesn't Everyone Have Tinnitus? (The Heavy Metal Lottery & The Perfect Storm)
A logical question comes up at this point: if mercury (from fish or amalgam), lead (from old pipes), etc. wreak such extreme destruction, why doesn't half of humanity have tinnitus immediately after a tuna pizza? The answer lies in our body's own protective shields and a true biological lottery — and in the fact that a tinnitus is almost never triggered by a single, isolated factor.
1. The toxicological lottery (the local weak point):
Heavy metals don't have a built-in GPS system for the ear. They circulate blindly in the blood and look for the place of least resistance (locus minoris resistentiae). Where they deposit themselves is often pure chance — and depends on where your body currently has a weak spot. If, for example, you grind your teeth heavily at night or have a silent inflammation in the neck-jaw area, the vascular permeability around your ear is extremely high. The so-called blood-labyrinth barrier, which is supposed to actually protect the ear, then sits wide open. The mercury finds this open door and deposits itself right there at the auditory nerve, while in another person it might just keep on wandering.
2. The body's own landfill, the glutathione protective shield, and the starting depot:
A healthy body produces massive amounts of glutathione in the liver — a molecule that handcuffs heavy metals like with chains and excretes them before they reach the ear. But here's the hard reality of exposure: some people — often completely unknowingly — come into massively more contact with heavy metals than others. Whether through contaminated air, old amalgam fillings in the mouth, the workplace, smoking, heavy-metal-containing foods, or constant contact with contaminated everyday objects. In the end, it's always a toxic mix of the sheer amount of exposure and the body's own ability to bind and excrete these poisons. If the body can't manage this, it often deposits poisons in supposedly safe „landfills“ (like bones or classic fat tissue) to pull them out of the bloodstream. And this is exactly where a fatal biological trap for our hearing hides: our nervous system — and especially the insulating myelin layer of the auditory nerve — is almost 80% pure fat. So when the body now desperately tries to „park“ lipophilic (fat-soluble) heavy metals in fat tissue, in the unfortunate interplay of the lottery it often hits exactly this highly sensitive nerve tissue, or the structures around the hair cells.
On top of that, there's a hard, often less commonly discussed biological fact: many people start the toxic lottery already filled with a heavy metal depot from the day they're born. Why? Because investigations suggest that during pregnancy, mothers pass on part of their own years-long accumulated heavy metal depots through the placenta to the fetus. For some people, the cellular barrel is already considerably fuller from the start.
It finally becomes dangerous when this protective system tips: through extreme stress, genetics, or nutrient deficiency, detoxification suddenly runs at its limits. The body's own depots open up, or the newly arriving poison doesn't get intercepted in the first place, circulates in the blood, and inevitably looks — like in the lottery mentioned earlier — for its weak point in the body.
3. The fatal mixed situation (the perfect storm):
In biological reality, though, we often see an extremely complex mixed picture here — and that also clears up the misunderstanding that everyone who gets a tinnitus after a noise event must automatically be completely poisoned with heavy metals. That's not the case.
What often happens is more like this: a person is already carrying a certain toxic baseline load — through environmental toxins or heavy metals in the hair cells, in their mitochondria, or directly at the auditory nerve. The myelin layer might already be slightly thinned, the calcium pumps already running closer to their limit, or the cells working hard at the threshold. By itself, this often doesn't trigger a permanent tinnitus at all. Your body buffers it and balances on a tightrope.
But then life adds the combination factor on top: you slip into a phase with extreme chronic stress. The stress hormones (adrenaline/cortisol) constrict the blood vessels, massively throttle blood flow to the ear, and rob you of restorative sleep. Your body can't recover overnight anymore. If you're now also exposed to a noise event in exactly this highly vulnerable state (whether an acute noise peak or chronic constant sound exposure), at some point in this chain the system finally tips. The pre-damaged hardware simply can't cushion this mechanical force anymore. The ion balance collapses, the actin scaffolding breaks down, or the myelin layer fails for good — and the electrical permanent signals can develop.
In my view, it's the fatal combination: the toxin delivers the slow weakening of the hardware, the stress cuts off the oxygen supply, and the noise is then often just the final drop that makes the already-full cellular barrel overflow.
In my view, of course, there's also the tinnitus at the other end of the spectrum, triggered purely by toxic medications or massive heavy metal poisoning. When the chemical dose (e.g., from aggressive chemotherapy or acute poisonings) is high enough, no „perfect storm“ is needed at all, and no additional noise event either. In those cases, the poison alone is more than enough to disable the cell power plants or damage the nerves.
Why Toxin-Induced Tinnitus (Heavy Metals & Pesticides) Is Often So Persistent
Anyone who avoids noise stops the trigger immediately. With toxin-induced tinnitus — and by that I specifically mean the load from real environmental toxins, pesticides, or heavy metals — that's often considerably more complicated. This form becomes so extremely tough and persistent especially when these substances actually turn out to be the main mechanism or a larger factor in the tinnitus event. That's because they literally embed themselves deep in the nerve tissue and in the cells. They don't simply disappear from the bloodstream after a few hours like a normal pain pill. They cling on, and the body can often only excrete these stubborn toxins extremely slowly, with great difficulty, and over a long period.
And What Can You Do Now?
And what can you do now? The scientific and clinical-practice evidence for the mechanisms described here can be found on my sources page. For anyone who wants to dive deeper and find out what, in my view and experience, concretely helps with medication- or toxin-induced tinnitus — just click the link below:
Important Notice
Never stop prescription medications on your own! For ear sounds related to taking medication — especially if they came on suddenly — please consult a physician promptly to clarify the next steps. Any change to your medication needs to happen under medical supervision.
The content, explanatory models, and strategies shared on this website are not medical advice, but my personal experience report and my own research. Every body is individual. I am not a doctor and make no promises of healing. For health complaints, please consult a qualified physician. Implementing the approaches described here is at your own responsibility.