Scientific Sources & Clinical Evidence
This page shows the foundation underneath everything I write on this website. My model is my personal interpretation of what happened cellularly with my own tinnitus. But the individual building blocks — the crosslinkers between actin filaments in the stereocilia, calpain activation under noise, ATP metabolism, XIRP2 repair, central gain in the brain, the local HPA axis in the cochlea, the mitochondrial action of Q10, B vitamins, and niacin — are not made up. They are documented in the research, and they are tested in clinical practice.
Introduction: Two kinds of evidence
An honest preface: I'm putting two kinds of evidence on this page, and I'm deliberately not blending them with hierarchical scoring.
First: the mechanism studies from basic research. These are peer-reviewed papers in journals like Nature Communications, Journal of Neuroscience, PNAS, or eLife. They show how the cellular machinery actually works — how crosslinkers stabilize the stereocilia, how calpains activate under noise, how XIRP2 makeshift-stabilizes breaks, how ATP elevation restores hearing after noise damage. These studies are essential for understanding the model.
Second: the clinical practice evidence from experienced physicians. These are voices like Dr. Lutz Wilden, who has been treating inner-ear patients with low-level laser therapy continuously since 1987 — that's over 35 years — keeping audiograms before and after treatment as standard documentation. Plus thousands of home-laser users worldwide who track their self-treatment with control audiometry. In Switzerland, Tinnitool has likewise treated thousands of patients since the 1990s with the same working logic (LLLT → ATP elevation in the hair cells). On top of that: the Hahn group in Prague (540 patients across two published studies), the LMU Munich group (Tauber et al.), the Italian groups (Cuda, Teggi, Piacenza), plus clinical studies from Iran, Japan, Brazil, Korea, and Qatar adding hundreds more patients. And Dr. Dietrich Klinghardt, with his decades of work on heavy metal and toxin loads. Most of this practical experience is not published in Nature Communications — and there are reasons for that, which Wilden himself talks about. But that doesn't change the fact that, over the past decades, a genuinely remarkable number of real patients have recovered along this path, with audiometric documentation.
Why both sources count
I think it's more honest to put both sources of evidence side by side than to pretend that "peer-reviewed only" equals truth. The reality is: a large share of tinnitus research funding flows into hearing aid development and patent-protected drug pipelines. For non-patentable nutrient combinations, for Wilden's specific high-dose laser protocol, for Klinghardt's detoxification protocols — there is simply no institutional research interest. That doesn't mean all of this works — and I'll say plainly, where I myself am not sure if something is broadly applicable. But it also doesn't mean that the absence of RCTs equals the absence of effect.
I am not a doctor, not a scientist, not a researcher. I am someone who lived through this — who recovered twice, with audiometric documentation — and who read, researched, and experimented obsessively. When I cite a study or a doctor here, that doesn't mean it proves my path will work for you. It means the individual building blocks I rely on are taken seriously in research and in clinical practice. For acute symptoms — especially acute tinnitus or hearing loss — please see an ENT physician first to rule out organic causes.
The common thread: ATP elevation = tinnitus improvement
Before I dive into the detail sections, I want to show you the central finding that runs underneath all of this. If there's only one thing you take away from this sources page, it should be this:
Whenever, anywhere in the world over the past decades — by whatever route — ATP production in the hair cells of the inner ear was specifically elevated, tinnitus improved.
This isn't theory and it isn't wishful thinking. It is the consistent finding of three completely independent therapy tracks, researched and applied by scientists and physicians in at least ten different countries, using different methods, in different patient cohorts. Here are the three tracks — all leading to the same biochemical endpoint.
Track 1: ATP elevation through laser light (Photobiomodulation / LLLT)
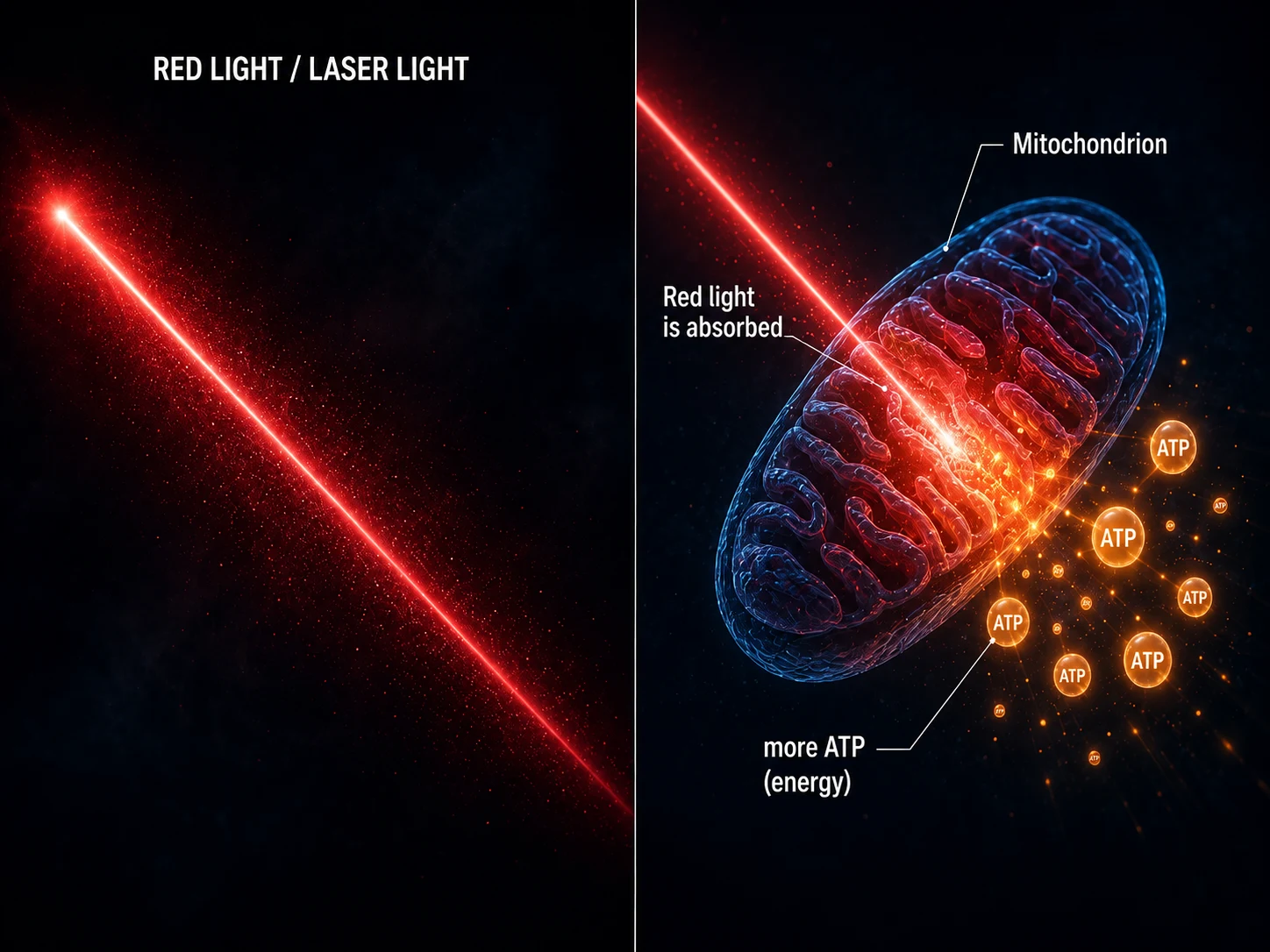
Laser light in the 600–900 nm range is absorbed by cytochrome c oxidase in the respiratory chain of the mitochondria. The biochemical effect: more ATP, less oxidative stress, the cell exits energetic emergency mode.
Key voices on this track:
- Tiina Karu, Russian Academy of Sciences, from 1981 onward — molecular mechanism proof, cytochrome c oxidase identified as the primary photoacceptor
- Dr. Lutz Wilden, Bad Füssing/Ibiza, since 1987 — thousands of tinnitus patients treated with high-dose 830 nm laser, audiometry documented, peer-reviewed publications, WALT Award 1998
- Hahn group, Charles University Prague, 2001/2012 — up to 420 patients, 56.7% objective tinnitus improvement with an average 30 dB gain
- Tauber et al., LMU Munich, 2003 — TCL system for transmeatal cochlear irradiation
- Cuda & De Caria, Italy, 2008 — combined counseling and LLLT
- Teggi et al., San Raffaele Milan, 2008/2009 — LLLT for Meniere's disease
- Mollasadeghi et al., Iran, 2013 — double-blind RCT in noise-induced tinnitus, significant
- Shiomi et al., Kyoto University, 1997 — 40 mW 830 nm transmeatal, pioneering work
- Panhóca et al., Brazil, 2023 — comparative RCT, LLLT identified as the most effective approach
→ Full detail: see Section 11 (Wilden) and Section 12 (International LLLT research).
Track 2: ATP elevation through pharmaceuticals (AC102)
A pharmacological compound developed in Berlin that intervenes directly in mitochondrial ATP production while simultaneously breaking down reactive oxygen species. The pharma industry is now picking up here what Wilden and Karu have been doing for decades — only in a patentable drug form.
Key voices on this track:
- Rommelspacher et al., AudioCure Pharma Berlin, PNAS 2024 — a single dose substantially improves hearing after acoustic trauma (13–31 dB recovery from an average 80 dB loss in the animal model), ATP production elevated, ROS reduced, synapses protected
- Tziridis et al., MDPI 2025 — ribbon synapses recover, tinnitus-specific behavioral patterns regress
- Nieratschker et al., Cell Death & Disease 2024 — also effective in cochlear implantation trauma
- Phase 2 clinical trial NCT05776459 — currently running across Europe in 200 SSNHL patients
Track 3: ATP elevation through nutrients
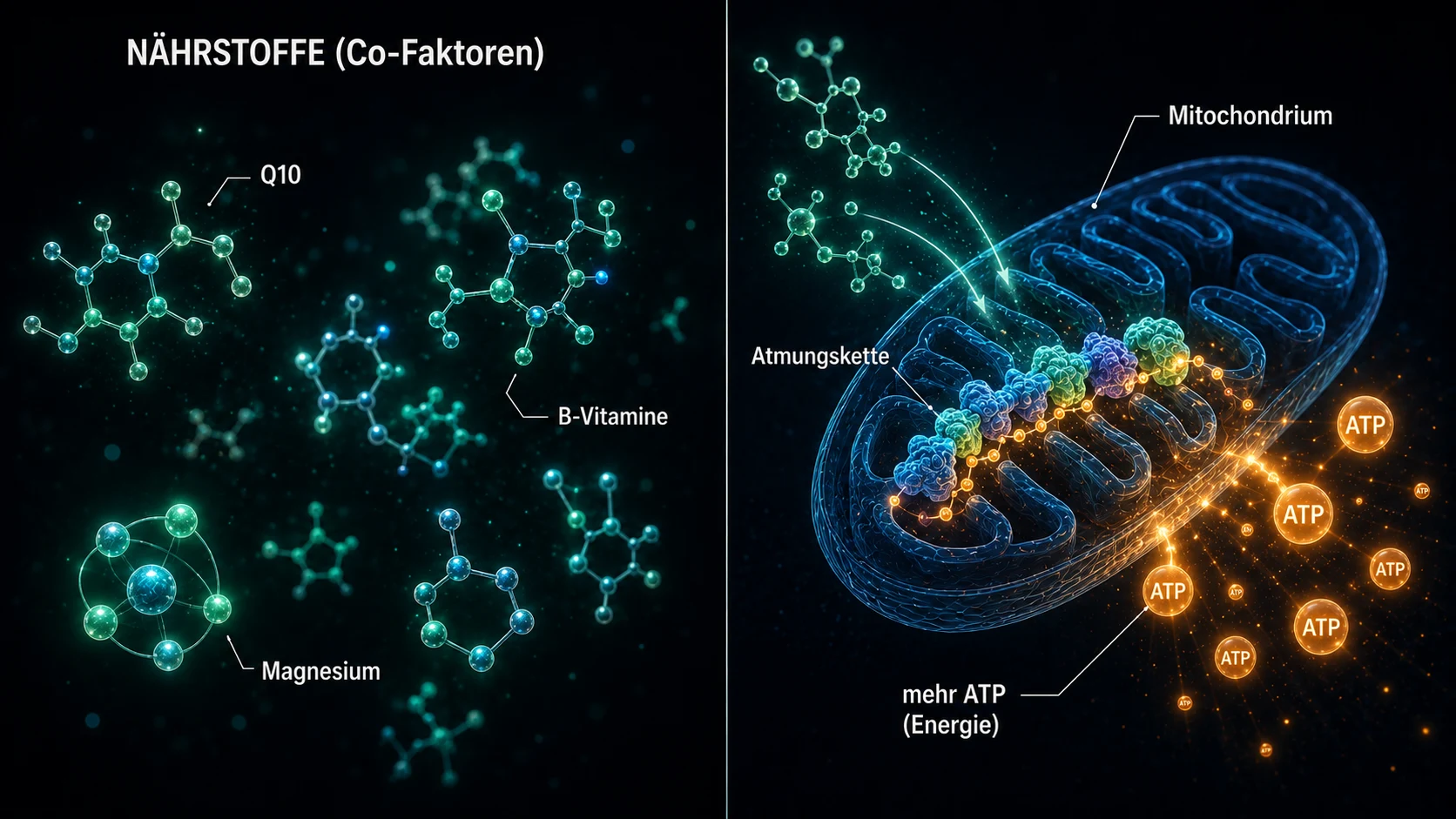
Mitochondrial cofactors that directly support or unlock the respiratory chain. Without enough Q10, electron transport between Complex I/II and Complex III doesn't run. Without enough B12, nerve fibers demyelinate, including the auditory nerve. Without enough magnesium, around 600 enzymatic reactions don't function — including ATP synthesis itself. Antioxidants like vitamin C, E, selenium, zinc, and alpha-lipoic acid protect the cell from the reactive oxygen species that pile up as a consequence of the energetic emergency mode.
3.1 Classical mitochondrial cofactors (Q10, magnesium, B12)
- Fetoni et al., Brain Research 2009 — Q10 significantly reduces apoptosis of outer hair cells after acoustic trauma
- Staffa et al., Noise & Health 2014 — Q10 shortens recovery time after noise exposure, reduces tinnitus
- Astolfi et al., PLOS One 2016 — Q10 plus multivitamin protects against cisplatin ototoxicity
- Cevette et al., Mayo Clinic 2011 — 532 mg magnesium over 3 months significantly reduces tinnitus burden (open-label, n=26, no placebo)
- Singh et al., Noise & Health 2016 — 42.5% of tinnitus patients have B12 deficiency; in those deficient, B12 substitution improves significantly
- Shemesh et al., 1993 — historical first description of the B12–tinnitus connection
→ Full detail: see Section 7 and Section 8.
3.2 Niacin / Vitamin B3 / NAD+ — the most direct ATP lever there is
The dosages referenced here come from published studies and are not recommendations for self-medication. Before any supplementation — especially at higher doses — talk to your doctor.
Niacin (vitamin B3, in its forms nicotinic acid, niacinamide, and nicotinamide riboside) is the direct metabolic precursor of NAD+ and NADH — the central coenzymes of the mitochondrial respiratory chain. Without enough NAD+, the Krebs cycle can't deliver electrons to the respiratory chain, and without those electrons, no ATP is produced. That makes niacin not just "another nutrient for tinnitus," but a direct lever for ATP production in the hair cells. If my model is right — chronic tinnitus as an energy crisis of the hair cell — then niacin supplementation should measurably help. And that's exactly what the research has been showing for over 80 years.
The niacin flush — and why it matters biologically
Anyone taking nicotinic acid for the first time (especially on an empty stomach, or in higher doses starting around 100 mg) will, within 15–30 minutes, experience the famous-infamous niacin flush: skin gets hot, tingles, turns red from face to chest, sometimes down to the thighs. Looks like a sunburn, feels like a heat wave trapped under the skin. Lasts 30–60 minutes, is harmless, and resolves on its own. The first time, you think: "I'm dying." The second time: "Ah, so this is the flush." The third time: "Honestly, not that bad."
Here's what's happening: nicotinic acid releases prostaglandin D2 in the body, which triggers massive vasodilation — the fine skin vessels open up, blood flow shoots up. The exact same thing happens in the fine vessels of the inner ear. This is not just a quirky side effect — it is part of the therapeutic mechanism:
Better microcirculation in the cochlea = better oxygen and nutrient supply to the hair cells = more energy for repair.
Atkinson 1944 used exactly this.
The pharmaceutical industry has, over recent decades, marketed "flush-free niacin" (niacinamide / nicotinamide) as a supposedly better-tolerated alternative — and it's true that many people do tolerate it better. But niacinamide does not have the vasodilation effect, and therefore has a much weaker microcirculation impact in the inner ear. Both forms convert to NAD+ in the body, but for tinnitus patients, the original nicotinic acid (with flush) tends to be more effective, because it pulls two levers simultaneously: NAD+ supply and inner-ear blood flow. That's also why almost all the historical tinnitus studies worked with nicotinic acid, not niacinamide.
Practical tips from the biohacker community:
- The flush is significantly reduced by an aspirin pre-dose (150–300 mg, 30 minutes ahead) — clarify with your doctor first whether aspirin is safe for you
- Over time, the body adapts and the flush weakens
- For low daily maintenance doses, un-buffered nicotinic acid taken after meals is the clean route
Historical studies — the flush as efficacy marker
The niacin flush isn't just a side effect — historically, it was the marker for the therapeutically sufficient dose. If the flush doesn't appear, the dose is too low. If it appears, you know the niacin is biologically active and the vasodilation is reaching the cochlea. That's exactly how the pioneers of niacin-based tinnitus therapy worked:
Atkinson M. (1941). Observations on the etiology and treatment of Meniere's syndrome. Journal of the American Medical Association, 116, 1753–1760.
Atkinson M. (1944). Meniere's syndrome: results of treatment with nicotinic acid in the vasoconstrictor group. Archives of Otolaryngology, 40, 101–107.
Atkinson M. (1944). Tinnitus aurium: observations on its nature and control. Annals of Otology, Rhinology, and Laryngology, 53, 742–751.
Atkinson M. (1947). Tinnitus aurium: some considerations on its origin and treatment. Archives of Otolaryngology, 45, 68–76. PMID: 20284478.
Atkinson M. (1948). Meniere's syndrome: observations on vitamin deficiency as the causative factor. II. The cochlear disturbances. Archives of Otolaryngology, 50, 564–588. PMID: 15393403.
Atkinson published a systematic series of papers on tinnitus, Meniere's disease, and nicotinic acid therapy across nearly two decades — in what were then the leading ENT journals. His central finding: in the "vasoconstrictor group" — meaning tinnitus patients whose symptoms traced back to circulatory issues in the inner ear — chronic nicotinic acid treatment in doses that triggered a flush led to long-term improvement in roughly half the patients. Initially as injection, later oral.
Flottorp G, Wille C. (1955). Nicotinic acid treatment of tinnitus: a clinical-audiological examination. Acta Oto-Laryngologica, 43(Suppl. 118), 85–99. PMID: 13227997. Link: PubMed
This is the study with the strongest methodological foundation. Flottorp and Wille didn't just gather subjective patient reports — they measured objective tinnitus loudness before and during niacin treatment using masking procedures. That means they played external tones to the patient at increasing volume and identified the threshold at which the external tone overrode the tinnitus. This "minimum masking level" is an objective metric for tinnitus intensity.
Their result: in the majority of Meniere's patients, tinnitus symptoms improved. And in a group of tinnitus patients with normal or near-normal hearing, almost all patients showed measurably lower tinnitus masking thresholds plus subjective improvement. So niacin didn't just make the tinnitus "feel" quieter — it made it objectively measurably quieter.
And the critical point: the effective doses were exactly the ones that triggered a flush. Patients who reached the flush benefited. Those who didn't — because the dose was too low, or because a flush-free form (niacinamide) was used — did not benefit.
Hulshof J, Vermeij P. (1987). The effect of nicotinamide on tinnitus: a double-blind controlled study. Clinical Otolaryngology, 12(3), 211–214. PMID: 2955964.
This study is often cited as evidence against niacin in tinnitus. It compared niacinamide (= flush-free niacin, no vasodilation) against placebo in 48 patients and found no effect. So the study used niacinamide instead of nicotinic acid — meaning the form without the vasodilation effect that was central to the positive studies. That explains the null result. Yet to this day, the study is cited in ENT reviews as evidence against niacin, without mentioning this methodological detail.
The Medscape overview article on tinnitus pharmacotherapy still acknowledges, even today:
"Niacin has been used as therapy for tinnitus for years with variable success… Patients often sustain a blush when taking niacin in effective doses… About half of all patients with tinnitus report successful treatment with niacin."
Source: medscape.com
In other words: even academically conservative US medicine acknowledges that around 50% of tinnitus patients improve under niacin — and that the flush is the marker for the effective dose. Yet in the German ENT mainstream, this has practically vanished. Eighty years after Atkinson, that's a remarkable memory gap.
Modern mechanism studies
Brown KD, Maqsood S, Huang J-Y, et al. (2014). Activation of SIRT3 by the NAD+ precursor nicotinamide riboside protects from noise-induced hearing loss. Cell Metabolism, 20(6), 1059–1068. PMID: 25470550. Link: PubMed
A high-profile mechanism study: nicotinamide riboside (NR) as an NAD+ precursor prevents noise-induced hearing loss and spiral ganglion neurite degeneration in mice — even when given after noise exposure. The mechanism runs through the mitochondrial sirtuin SIRT3, an NAD+-dependent enzyme that reduces oxidative stress. Direct molecular evidence that NAD+ elevation protects hair cells from noise damage.
Han S, Du Z, Liu K, Gong S. (2020). Nicotinamide riboside protects noise-induced hearing loss by recovering the hair cell ribbon synapses. Neuroscience Letters, 725, 134910. PMID: 32171805. Link: PubMed
From Beijing Friendship Hospital, Capital Medical University. NR supplementation restores the ribbon synapses between hair cells and auditory nerve after noise trauma — in mice — meaning the very structures whose loss is, in current understanding, a co-driver of chronic tinnitus (Hidden Hearing Loss).
Wang B, Chen S, Yang Z, et al. (2024). Personalized Porous Gelatin Methacryloyl Sustained-Release Nicotinamide Protects Against Noise-Induced Hearing Loss. Advanced Science. PMC10966548. Link: PMC
Direct confirmation of the ATP model: this study shows that noise trauma in cochlear hair cells and spiral ganglion neurons reduces NAD+ levels and triggers mitochondrial dysfunction. Nicotinamide supplementation restores mitochondrial homeostasis and prevents neurotoxic damage — both in vitro and in vivo. That's exactly the logic of my model, confirmed in a top-tier 2024 publication.
Clinical correlation studies
Igarashi M, Nakagawa-Nagahama Y, Miura M, et al. (2022). Blood levels of nicotinic acid negatively correlate with hearing ability in healthy older men. NPJ Aging, 8(1):5. PMC9933288. Link: PMC
42 older Japanese men (>65 years): lower blood levels of nicotinic acid correlate significantly with elevated hearing thresholds at 1000 and 2000 Hz. Translation: less niacin in your blood, worse hearing. First clinical confirmation in humans that NAD+ metabolism is directly tied to hearing ability.
Sun Y et al. (2024). L-shaped relationship between dietary niacin intake and hearing loss in United States adults: National Health and Nutrition Examination Survey. Frontiers in Nutrition. PMC11856504. Link: PMC
NHANES data 2011–2012 and 2015–2016, US adults aged 20–69: low dietary niacin intake is significantly associated with hearing loss. Population-level confirmation in the US.
Lee DY et al. (2018). Nutritional Status and Tinnitus. Clinical and Experimental Otorhinolaryngology. Link: e-ceo.org
Korean study: low intake of vitamin B2 and B3 was significantly associated with tinnitus distress, especially in the 66–80 age group.
Active clinical trial
ClinicalTrials.gov NCT05849519 — Active randomized controlled trial from China studying "Coenzyme I" (NAD+) injection in sudden hearing loss with tinnitus. Results pending, but the fact that NAD+ is being investigated as an injectable therapeutic for sudden hearing loss / tinnitus at all signals that the ATP / NAD+ model has arrived in mainstream academic research. Link: clinicaltrials.gov/study/NCT05849519
Summary: Niacin / NAD+
Niacin is the longest clinical tradition of any ATP-oriented tinnitus therapy — Atkinson 1944, Flottorp & Wille 1955. Plus modern mechanism confirmation in animal models (Brown 2014, Han 2020, Wang 2024) and in population studies (Igarashi 2022, NHANES 2024). The fact that mainstream medicine has largely forgotten this over the past decades isn't due to lack of evidence — it's due to the well-known industry pattern: a cheap vitamin can't be patented.
3.3 Clinical studies with micronutrient combinations
Wong AP, Kalinovsky T, Niedzwiecki A, Rath M. (2015). Pilot study on the effects of vitamin treatment in patients with tinnitus. Pilot study from the Dr. Rath Research Institute (Santa Clara, USA), published on the institute's website, not in a peer-reviewed journal. Link: drrathresearch.org
Clinical pilot study in 18 tinnitus patients between 44 and 85 years old, all with chronic tinnitus of at least three months' duration, conducted in collaboration with ENT specialists. Four months of daily supplementation with a specific vitamin and micronutrient combination, on top of physician-prescribed standard therapy. Hearing measurements with clinical audiometry at monthly intervals.
Results after 4 months:
- 30% of patients: mild hearing improvement (up to 10 dB)
- 45% of patients: clear hearing improvement (10–20 dB)
- 25% of patients: strong hearing improvement (20–50 dB), nearly normal hearing returning
- Over 75% of patients: reduction in ear noise
- In more than 50% of patients: tinnitus significantly reduced or completely gone
Small study, clearly positive results, conducted in collaboration with ENT specialists. Exactly the picture my own model predicts.
Petridis P, Korres GS, Gazouli M, et al. (2020). The Effect of Antioxidant Supplementation in Patients with Tinnitus and Normal Hearing or Hearing Loss: A Randomized, Double-Blind, Placebo Controlled Trial. Antioxidants, 8(11):554. PMC6950042. Link: ncbi.nlm.nih.gov
Double-blind randomized placebo-controlled study from Athens, with antioxidant supplementation (multivitamin plus alpha-lipoic acid) in tinnitus patients. Methodologically clean.
Kaya H, Koç AK, Sayın İ, et al. (2015). Vitamins A, C, and E and selenium in the treatment of idiopathic sudden sensorineural hearing loss. European Archives of Oto-Rhino-Laryngology, 272(5), 1119–1125.
70 sudden hearing loss patients received, in addition to standard therapy, a high-dose vitamin cocktail over 30 days: 400 mg vitamin C, 56,000 IU vitamin A, 400 IU vitamin E, and 100 µg selenium daily. Over 85% of these patients also reported tinnitus. Compared with 56 patients on standard therapy alone (methylprednisolone, trimetazidine, hyperbaric oxygen). The vitamin group showed significantly better hearing improvement.
Heidelberg ENT cohort study 2009 — A cohort study by a Heidelberg ENT physician (HNO 2009; 57:3) showed that sudden hearing loss / tinnitus patients who received micronutrients in addition to standard therapy achieved less hearing loss and a markedly higher rate of full remission than the standard-therapy-only group.
3.4 Clinical practitioners on Track 3
Just as Dr. Wilden is the best-known clinical practitioner on Track 1 (LLLT), there are established ENT physicians on Track 3 (nutrients) who have been implementing this strategy in their practices for years — usually as a private-pay service, because statutory health insurance doesn't reimburse it.
Dr. med. Gerd Hadrich, ENT specialist with a practice in Salzgitter, Germany, has for years offered vitamin protocols and infusion therapies specifically for tinnitus, sudden hearing loss, and vertigo. His concept: vitamins, trace elements, amino acids, blood salts, and — particularly interesting — "catalysts of the citric acid cycle."
The citric acid cycle (Krebs cycle) is precisely the metabolic stage in the mitochondria that supplies NADH and FADH₂ as electron donors for ATP production in the respiratory chain. Which means: Hadrich is directly injecting the substances that drive ATP production in the inner-ear cells. That is Track 3 in its purest form, carried out by a practicing ENT specialist in Germany.
→ Practice profile: Dr. Hadrich, ENT Salzgitter
Hadrich is not the only one. Several ENT practices in the German-speaking region today offer high-dose vitamin C infusions, micronutrient cocktails, and antioxidant therapies for tinnitus and sudden hearing loss — as private-pay services, because standard guidelines and insurance reimbursement lag behind the international research landscape. Once you develop an eye for it, you'll see a growing German ENT practice network that quietly and consistently runs Track 3.
What the three tracks together mean
Three completely independent therapy tracks, developed in different countries, by different research traditions, using different methods — and all three converge on the same biochemical endpoint: elevated ATP production in the mitochondrial respiratory chains of the hair cells.
If this were coincidence, you'd have to explain why Russians with lasers, Berlin pharma researchers with pyridoindoles, Norwegian ENT physicians with niacin, and German ENT practitioners with micronutrient infusions all independently land on the same biochemical lever. It is not coincidence. It is convergent evidence at the highest level.
The three tracks don't contradict each other — they complement each other. Anyone optimizing therapy probably combines them. That's exactly what I describe on my approach page.
Part 1: Mechanism Studies from Basic Research
Crosslinkers between the actin filaments in stereocilia
On the main page I compare the stereocilia to a bundle of uncooked spaghetti held together by short protein bridges — the crosslinkers. These crosslinkers aren't something I made up. They are three concrete protein families — Plastin/Fimbrin (PLS1), Espin (ESPN), and Fascin-2 (FSCN2) — and their existence and function in the stereocilia have been molecularly documented for over 20 years.
Krey JF, Krystofiak ES, Dumont RA, et al. (2016). Plastin 1 widens stereocilia by transforming actin filament packing from hexagonal to liquid. Journal of Cell Biology, 215(4), 467–482. DOI: 10.1083/jcb.201606036. PMID: 27811163. Link: pmc.ncbi.nlm.nih.gov
The key study quantifying the crosslinkers. Using mass spectrometry, Krey et al. demonstrated that a single stereocilium contains roughly 30,500 plastin-1 molecules, 16,100 fascin-2 molecules, and 14,800 espin molecules between the actin filaments. After actin itself, plastin-1 is the second-most-abundant protein in the entire stereocilium. Mice lacking functional plastin-1 or fascin-2 showed reduced hearing function; double mutants were the most severely affected. Stereocilia without plastin-1 are shorter and thinner than wildtype stereocilia. That's the direct experimental proof that the crosslinkers actually carry the structural integrity of the stereocilia.
Perrin BJ, Strandjord DM, Narayanan P, et al. (2013). β-Actin and Fascin-2 Cooperate to Maintain Stereocilia Length. Journal of Neuroscience, 33(19), 8114–8121. DOI: 10.1523/JNEUROSCI.0238-13.2013. PMID: 23658152. Link: pubmed.ncbi.nlm.nih.gov
Direct evidence of what happens when fascin-2 doesn't function properly: mice with a fascin-2 mutation show progressive, high-frequency hearing loss and a specific shortening of the second and third rows of stereocilia. The mutant fascin-2 variant still binds to actin, but can no longer effectively crosslink the filaments — and that's exactly why the stereocilia lose their length. That's the same structural endpoint I describe on the main page for noise-induced crosslinker loss, just simulated here through a genetic mutation rather than calpain cleavage.
Sekerková G, Zheng L, Loomis PA, et al. (2004). Espins are multifunctional actin cytoskeletal regulatory proteins in the microvilli of chemosensory and mechanosensory cells. Journal of Neuroscience, 24(23), 5445–5456. DOI: 10.1523/JNEUROSCI.1279-04.2004. PMID: 15190118. Link: pubmed.ncbi.nlm.nih.gov
The structural characterization of espin as an actin crosslinker in stereocilia. Espin is identified as a bundling protein for the parallel actin filaments and is not inhibitable by calcium — which matters, because the interior of the stereocilia is exposed to calcium fluctuations during normal function. Mice with defective espins are deaf and have balance disorders. Espin mutations also cause inherited deafness in humans.
What this all means together: If the three crosslinkers — plastin/fimbrin, espin, fascin-2 — already produce hearing loss and structural stereocilia defects through genetic mutation or knockout, it is biologically plausible that an acquired, noise-induced calpain cleavage of these or related crosslinkers — as I describe on the main page — could produce the same structural endpoint.
Calpain activation under noise
Under noise, calcium floods massively into the hair cell. This calcium overload activates calpains — calcium-dependent protease enzymes that subsequently cleave actin-crosslinking proteins. That this mechanism is real has been documented by two independent research labs using different calpain inhibitors.
Lai R, Fang Q, Wu F, Pan S, Haque K, Sha SH. (2023). Prevention of noise-induced hearing loss by calpain inhibitor MDL-28170 is associated with upregulation of PI3K/Akt survival signaling pathway. Frontiers in Cellular Neuroscience, 17, 1199656. DOI: 10.3389/fncel.2023.1199656. Link: pmc.ncbi.nlm.nih.gov
Direct evidence for the calpain mechanism: noise activates µ-calpain and m-calpain in the hair cells, and the calpain inhibitor MDL-28170 prevents both hearing loss and synapse loss. The study additionally shows that calpain cleaves the structural protein α-fodrin — a spectrin-actin crosslinker in the cellular cortex. That's not exactly the same crosslinker type as the stereocilia-specific plastin/espin/fascin-2, but it confirms that calpain activates under noise and attacks actin-crosslinking proteins. That the stereocilia crosslinkers might also be affected is a plausible hypothesis arising from this convergence.
Yamaguchi T, Yoneyama M, Ogita K. (2017). Calpain inhibitor alleviates permanent hearing loss induced by intense noise by preventing disruption of gap junction-mediated intercellular communication in the cochlear spiral ligament. European Journal of Pharmacology, 803, 187–194. DOI: 10.1016/j.ejphar.2017.03.058. PMID: 28366808. Link: pubmed.ncbi.nlm.nih.gov
Confirms the calpain damage mechanism from a second lab using a different inhibitor (PD150606). Extends the picture to a second site of damage: under noise, calpain also attacks gap junction communication in the spiral ligament — the lateral cochlear wall. Noise damage is never confined to a single location.
Background reading: Fettiplace R, Hackney CM. (2006). The sensory and motor roles of auditory hair cells. Nature Reviews Neuroscience, 7(1), 19–29. — The classic overview of hair cell architecture and function.
Actin repair through XIRP2 (Phase 1)
Wagner EL, Im JS, Sala S, et al. (2023). Repair of noise-induced damage to stereocilia F-actin cores is facilitated by XIRP2 and its novel mechanosensor domain. eLife, 12, e72681. DOI: 10.7554/eLife.72681. PMID: 37294664. Link: elifesciences.org/articles/72681
The key mechanistic paper on hair cell self-repair. Under noise, measurable "gaps" form in the actin scaffold of the stereocilia. In mice, these gaps are closed within a week by freshly synthesized γ-actin. The repair protein XIRP2 mechanically detects the damage and initiates the repair. Without XIRP2, the damage remains permanent.
On the main page I describe XIRP2 as "duct tape" that makeshift-stabilizes the breaks (Phase 1). The actual Phase 2 repair — building fresh actin, inserting new crosslinkers — takes about a week in this study, in perfectly cared-for laboratory mice. I describe what that means for a stressed adult human, simultaneously stuck in the energetic hamster wheel, on the Mouse Misread page.
NIH-funded (R01DC021176).
ATP elevation as a repair lever: AC102
This is the centerpiece of my noise protocol on the pharmacological track: when the cell doesn't have enough energy, it can't repair itself. Here are the studies showing that this idea is being taken seriously — a Berlin pharmaceutical company is currently developing a drug that targets exactly this mechanism.
Rommelspacher H, Bera S, Brommer B, Ward R et al. (2024). A single dose of AC102 restores hearing in a guinea pig model of noise-induced hearing loss to almost prenoise levels. Proceedings of the National Academy of Sciences (PNAS), 121(15), e2314763121. PMID: 38557194. Link: pmc.ncbi.nlm.nih.gov
The core study on AC102. In vitro tests showed that AC102 substantially elevates cellular ATP production while simultaneously breaking down reactive oxygen species (ROS). In the animal model, a single dose significantly improved hearing after noise trauma — described in the study title as "almost to prenoise levels" (specifically: 13–31 dB improvement against an average noise-induced hearing loss of 80 dB — significant, but not full restoration). The mechanisms — driving up ATP production, reducing ROS, protecting synapses — are exactly the mechanics of my model, just pharmacologically forced.
Tziridis K, Rasheed J, Kwiatkowska M, et al. (2025). A Single Dose of AC102 Reverts Tinnitus by Restoring Ribbon Synapses in Noise-Exposed Mongolian Gerbils. International Journal of Molecular Sciences, 26(11), 5124. Link: mdpi.com
This study additionally tested whether AC102 also reverses tinnitus-specific behavioral patterns. Result: yes, largely — and the ribbon synapses between hair cells and auditory nerve recovered significantly. Direct evidence that the continuous glutamate firing at the auditory nerve stops once cellular energy comes back.
Nieratschker M, Yildiz E, Gerlitz M, et al. (2024). A preoperative dose of the pyridoindole AC102 improves the recovery of residual hearing in a gerbil animal model of cochlear implantation. Cell Death & Disease, 15, 531. DOI: 10.1038/s41419-024-06854-9. Link: nature.com
Extends the AC102 evidence to a second damage track: the compound also protects residual hearing in cochlear implantation trauma. That shows the mechanism works independently of the damage trigger — whether mechanical trauma from noise or from a surgery, the cellular emergency cascade is the same, and the ATP lever functions in both cases.
AudioCure Pharma GmbH. Clinical Study NCT05776459. AC102 is currently in a Europe-wide Phase 2 study in patients with sudden sensorineural hearing loss (SSNHL) — approximately 200 patients, recruitment running through end of 2025. Link: clinicaltrials.gov/study/NCT05776459
Stress, the HPA axis, and the cochlea as a neuroendocrine organ
Stress-related tinnitus is scientifically harder to pin down than noise-induced tinnitus, but the underlying principle — that chronic stress can act directly on the cochlea via the HPA axis — has been well-researched for about 15 years. The key insight: the cochlea itself has a complete, local HPA system. It isn't only a receiver of systemic stress hormones — it produces them locally.
Graham CE, Vetter DE. (2011). The mouse cochlea expresses a local hypothalamic-pituitary-adrenal equivalent signaling system and requires corticotropin-releasing factor receptor 1 to establish normal hair cell innervation and cochlear sensitivity. Journal of Neuroscience, 31(4), 1267–1278. DOI: 10.1523/JNEUROSCI.4545-10.2011. PMID: 21273411. Link: pubmed.ncbi.nlm.nih.gov
The key study. The mouse cochlea expresses the entire HPA-axis signaling system locally: corticotropin-releasing factor (CRF), CRF1 receptor, ACTH, mineralocorticoid receptor, and glucocorticoid receptor. Mice with knockout of the CRF1 receptor show disrupted hair cell innervation and reduced cochlear sensitivity. That's the mechanistic proof that stress can act not just through the brain, but directly at the ear.
Graham CE, Basappa J, Vetter DE. (2010). A corticotropin-releasing factor system expressed in the cochlea modulates hearing sensitivity and protects against noise-induced hearing loss. Neurobiology of Disease, 38(2), 246–258. PMID: 20109547. Link: pubmed.ncbi.nlm.nih.gov
The predecessor study to Graham/Vetter 2011: shows that the local CRF system in the cochlea modulates hearing sensitivity and can protect against noise-induced hearing loss.
Furuta H, Mori N, Sato C, et al. (1994). Mineralocorticoid type I receptor in the rat cochlea: mRNA identification by polymerase chain reaction (PCR) and in situ hybridization. Hearing Research, 78(2), 175–180. PMID: 7982810. Link: pubmed.ncbi.nlm.nih.gov
The historical first description: mineralocorticoid receptors are expressed in the stria vascularis of the cochlea — meaning right inside the "battery" of the inner ear that maintains the potassium reservoir of the endolymph. Cortisol can modulate potassium secretion at that site via the mineralocorticoid receptors. That's the mechanistic bridge between psychological stress and a peripheral inner-ear effect.
Mazurek B, Haupt H, Olze H, Szczepek AJ. (2012). Stress and tinnitus – from bedside to bench and back. Frontiers in Systems Neuroscience, 6, 47. DOI: 10.3389/fnsys.2012.00047. Link: frontiersin.org
The systematic synthesis from the Berlin Charité: Mazurek and Szczepek consolidate the original findings of Graham/Vetter and Furuta into three testable hypotheses for how stress can trigger tinnitus — through the local HPA system of the cochlea, through cortisol modulation of mineralocorticoid receptors in the stria vascularis (with consequences for potassium secretion), and through glutamate-mediated plasticity in the auditory pathway.
Hébert S, Lupien SJ. (2007). The sound of stress: Blunted cortisol reactivity to psychosocial stress in tinnitus sufferers. Neuroscience Letters, 411(2), 138–142. DOI: 10.1016/j.neulet.2006.10.028. PMID: 17084027. Link: pubmed.ncbi.nlm.nih.gov
Tinnitus patients show a delayed and blunted cortisol response to acute psychosocial stress — a sign of a chronically depleted HPA axis. The same pattern shows up in ME/CFS and burnout. In my own life, that's exactly what happened — the HPA depletion came before the tinnitus, not the other way around.
Manohar S, Chen GD, Li L, Liu X, Salvi R. (2023). Chronic stress induced loudness hyperacusis, sound avoidance and auditory cortex hyperactivity. Hearing Research, 431, 108726. DOI: 10.1016/j.heares.2023.108726. PMID: 36905854. Link: pubmed.ncbi.nlm.nih.gov
Direct experimental evidence: rats under chronic cortisol stress develop hyperacusis behavior and tinnitus-like patterns in the auditory cortex — without any acute noise exposure. Supports the stress channel as a standalone entry route.
Schaette R, McAlpine D. (2011). Tinnitus with a Normal Audiogram: Physiological Evidence for Hidden Hearing Loss and Computational Model. Journal of Neuroscience, 31(38), 13452–13457. DOI: 10.1523/JNEUROSCI.2156-11.2011. Link: jneurosci.org
The foundation for the central gain model: when auditory input is reduced, the central auditory system raises its sensitivity — and produces tinnitus as amplified noise.
Auerbach BD, Rodrigues PV, Salvi RJ. (2014). Central Gain Control in Tinnitus and Hyperacusis. Frontiers in Neurology, 5, 206.
Overview of the central gain concept: the brain compensates for peripheral input loss with central amplification — with tinnitus and hyperacusis as side effects.
Eggermont JJ, Roberts LE. (2004). The neuroscience of tinnitus. Trends in Neurosciences, 27(11), 676–682.
A classic. Tinnitus correlates with altered spontaneous neural activity and altered tonotopic organization in the auditory cortex.
Trauma, stored stress, and the neuronal co-activation of neighboring pathways
The previous section shows how chronic stress can act directly at the inner ear via the HPA axis. But that's only part of the picture. The second part — at least equally important — concerns the question: how can stored trauma still trigger physical symptoms years later, and how can a local, autonomous stress focus in the brain actually co-activate neighboring nerve centers?
This is exactly the mechanism that Michael Prgomet describes didactically as an "electrostatic tension field" (see Section 14). On my Stress-Induced Tinnitus page I built up the model in plain language. This section shows: the individual neurobiological building blocks underneath that model are scientifically well-established. What's original about the synthesis is the connection of those building blocks into a coherent explanatory model — the individual mechanisms themselves are peer-reviewed and replicated multiple times.
5.1.1 Trauma leaves measurable neurobiological traces
A severe or chronic stress experience demonstrably changes the structure and function of certain brain regions. Trauma doesn't stay "just psychological" — it gets physically wired into the nervous system.
McEwen BS, Nasca C, Gray JD. (2016). Stress Effects on Neuronal Structure: Hippocampus, Amygdala, and Prefrontal Cortex. Neuropsychopharmacology, 41(1), 3–23. DOI: 10.1038/npp.2015.171. PMID: 26076834. Link: nature.com
Describes how chronic stress triggers measurable structural and functional changes in the hippocampus, amygdala, and prefrontal cortex. These are precisely the regions central to memory, fear, evaluation, and stress regulation — meaning exactly the structures involved in a persistently active stress pattern.
Sherin JE, Nemeroff CB. (2011). Post-traumatic stress disorder: the neurobiological impact of psychological trauma. Dialogues in Clinical Neuroscience, 13(3), 263–278. PMID: 22034143. Link: tandfonline.com
Overview of long-term neurobiological trauma effects: amygdala hyperreactivity, prefrontal control deficits, hippocampal changes, and lasting alterations in stress hormone systems. So trauma isn't "over the moment the situation is over" — it's wired into the nervous system.
Yehuda R, LeDoux J. (2007). Response Variation following Trauma: A Translational Neuroscience Approach to Understanding PTSD. Neuron, 56(1), 19–32. PMID: 17920012. Link: pubmed.ncbi.nlm.nih.gov
Shows that trauma can cause long-term changes in the HPA axis, the noradrenergic system, autonomic reactivity, and hippocampal function. That's the mechanistic foundation for stored stress patterns that can keep running quietly in the background.
5.1.2 Allostatic load — why only chronic stress becomes problematic
Acute, situational stress is healthy and easy for the body to absorb. The phenomena I describe on the Stress-Induced Tinnitus page don't show up in a normal argument or an acute strain — they emerge only when the system can no longer recover and the burden accumulates over time.
McEwen BS. (1998). Stress, Adaptation, and Disease: Allostasis and Allostatic Load. Annals of the New York Academy of Sciences, 840(1), 33–44. PMID: 9629234. Link: wiley.com
Establishes the concept of allostatic load. Acute stress is useful; chronic, cumulative load damages the system. That's the precise distinction my model relies on against the misleading claim that "stress causes tinnitus in general." It's not about everyday stress — it's about chronically pre-loaded systems.
McEwen BS, Stellar E. (1993). Stress and the individual: mechanisms leading to disease. Archives of Internal Medicine, 153(18), 2093–2101. PMID: 8379800.
Describes the mechanisms by which chronic stress leads to disease — through cumulative load, not through individual episodes. Clearly explains why not everyone with everyday stress develops these phenomena, but only those whose system is already chronically destabilized.
5.1.3 Central sensitization — the amplifier in a pre-loaded nervous system
Under chronic load, the central nervous system becomes more reactive to stimuli. Inhibition drops, excitability rises, stimulus thresholds fall. Previously sub-threshold stimuli are suddenly enough to trigger symptoms. That's the scientific description of what I call a "pre-loaded, stimulus-open system" on the Stress-Induced Tinnitus page.
Woolf CJ. (2011). Central sensitization: Implications for the diagnosis and treatment of pain. Pain, 152(3 Suppl), S2–S15. DOI: 10.1016/j.pain.2010.09.030. PMID: 20961685. Link: pubmed.ncbi.nlm.nih.gov
Defines central sensitization as elevated reactivity of central neurons to normal or sub-threshold input stimuli. An established cornerstone of modern pain research. My model transfers this principle to stress-induced tinnitus.
Latremoliere A, Woolf CJ. (2009). Central sensitization: a generator of pain hypersensitivity by central neural plasticity. The Journal of Pain, 10(9), 895–926. DOI: 10.1016/j.jpain.2009.06.012. PMID: 19712899. Link: pubmed.ncbi.nlm.nih.gov
Detailed description of the cellular and molecular mechanisms of central sensitization. Shows how a pre-loaded system creates the very precondition for small stress fields to become symptomatic.
Yunus MB. (2008). Central sensitivity syndromes: a new paradigm and group nosology for fibromyalgia and overlapping conditions. Seminars in Arthritis and Rheumatism, 37(6), 339–352. PMID: 18191990. Link: pubmed.ncbi.nlm.nih.gov
Applies the concept of central sensitization to fibromyalgia, chronic fatigue, irritable bowel syndrome, chronic tinnitus, and related syndromes. That's exactly the bridge my stress-tinnitus model rests on scientifically.
5.1.4 Ephaptic coupling — direct electrical co-activation of neighboring nerve cells
This is the hard neurophysiological core behind the Van de Graaff metaphor. When a neuronal area fires strongly and synchronously, it generates local electrical fields that can actually influence neighboring nerve cells — without a classical synapse. With sufficient activity, these fields can push neighboring cells over the firing threshold and synchronize their firing behavior. That is exactly the mechanism behind "nerve A fires, nerve B gets pulled along."
Anastassiou CA, Perin R, Markram H, Koch C. (2011). Ephaptic coupling of cortical neurons. Nature Neuroscience, 14(2), 217–223. DOI: 10.1038/nn.2727. PMID: 21240273. Link: nature.com
Direct experimental evidence of ephaptic coupling in the cortex. The study showed that extracellular electrical fields can alter the membrane voltage of neighboring neurons and synchronize action potential timing. This is the central proof that a strongly active group of nerve cells can in fact electrically co-activate neighboring cells.
Buzsáki G, Anastassiou CA, Koch C. (2012). The origin of extracellular fields and currents — EEG, ECoG, LFP and spikes. Nature Reviews Neuroscience, 13(6), 407–420. DOI: 10.1038/nrn3241. PMID: 22595786. Link: nature.com
Foundational overview of how electrical fields originate in the brain. Describes how synchronously active neuron groups can functionally influence other neurons through voltage gradients. Makes one thing clear: these are not "big lightning bolts" like a high-voltage generator — they are small, locally bound field effects, but they are real and biologically active.
Fröhlich F, McCormick DA. (2010). Endogenous electric fields may guide neocortical network activity. Neuron, 67(1), 129–143. DOI: 10.1016/j.neuron.2010.06.005. PMID: 20624597. Link: pubmed.ncbi.nlm.nih.gov
Shows that endogenous electrical fields don't just accompany neural network activity — they help drive it causally. Final nail in the coffin for the assumption that electrical field effects in the brain are merely incidental.
5.1.5 Kindling — repeated stimulation grooves the pattern in
When a neural area is repeatedly stimulated below threshold, over time it becomes easier and easier to activate — and increasingly recruits neighboring areas. Established in epilepsy research, by now also transferred to chronic pain, trauma, and stress states.
Goddard GV, McIntyre DC, Leech CK. (1969). A permanent change in brain function resulting from daily electrical stimulation. Experimental Neurology, 25(3), 295–330. PMID: 4981856.
The classic original paper on the kindling phenomenon. Repeated sub-threshold stimulation produces a permanent change in brain function — the area becomes easier and easier to activate over time.
Post RM. (2007). Kindling and sensitization as models for affective episode recurrence, cyclicity, and tolerance phenomena. Neuroscience & Biobehavioral Reviews, 31(6), 858–873. DOI: 10.1016/j.neubiorev.2007.04.003. PMID: 17555817. Link: pubmed.ncbi.nlm.nih.gov
Transfers the kindling concept to affective disorders, PTSD, and chronic stress states. Scientifically explains why chronically reactivated stress patterns don't fade over time but can grow stronger and broader — exactly the phenomenon I describe on the Stress-Induced Tinnitus page.
5.1.6 Glia activation and neuroinflammation — the biochemical amplifier
Chronic stimulation activates microglia and astrocytes. They release messenger substances (TNF-α, IL-1β, IL-6) that measurably elevate the excitability of surrounding neurons — and as a result push the entire region into a more reactive state. This is the biochemical amplifier between "pre-loaded system" and "stress field can break through."
Ji RR, Nackley A, Huh Y, Terrando N, Maixner W. (2018). Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology, 129(2), 343–366. DOI: 10.1097/ALN.0000000000002130. PMID: 29462012. Link: pubmed.ncbi.nlm.nih.gov
Direct evidence of how glia activation drives central sensitization. Microglia and astrocytes are not just passive support cells — they actively modulate neuronal excitability and, under chronic load, can shift nervous tissue into a permanently more stimulus-open state.
Michopoulos V, Powers A, Gillespie CF, Ressler KJ, Jovanovic T. (2017). Inflammation in Fear- and Anxiety-Based Disorders: PTSD, GAD, and Beyond. Neuropsychopharmacology, 42(1), 254–270. DOI: 10.1038/npp.2016.146. PMID: 27510423. Link: nature.com
PTSD and chronic anxiety are linked to measurable inflammatory changes in the nervous system. Closes the loop: trauma → stress → neuroinflammation → more stimulus-open tissue → easier activation of stored stress patterns.
5.1.7 Thalamocortical dysrhythmia — direct connection to tinnitus
In chronic tinnitus, MEG and EEG studies show pathological oscillation patterns between the thalamus and the auditory cortex. A locally altered activity pattern produces persistent theta-gamma couplings that can contribute to the lasting perception of a tone. That is the direct neurophysiological bridge between an overactive stress field and a persistent tinnitus perception.
Llinás RR, Ribary U, Jeanmonod D, Kronberg E, Mitra PP. (1999). Thalamocortical dysrhythmia: A neurological and neuropsychiatric syndrome characterized by magnetoencephalography. Proceedings of the National Academy of Sciences, 96(26), 15222–15227. DOI: 10.1073/pnas.96.26.15222. PMID: 10611366. Link: pnas.org
Establishes the concept of thalamocortical dysrhythmia as a mechanism for chronic neurological symptoms — measured with high-sensitivity MEG technology. The same kind of MEG instruments that can also make very small, locally bound voltage fields in the brain visible.
De Ridder D, Vanneste S, Langguth B, Llinás R. (2015). Thalamocortical Dysrhythmia: A Theoretical Update in Tinnitus. Frontiers in Neurology, 6, 124. DOI: 10.3389/fneur.2015.00124. PMID: 26106362. Link: frontiersin.org
Direct application of the concept to chronic tinnitus, with MEG data. Shows that pathological theta-gamma couplings in the auditory cortex are measurable in chronic tinnitus patients.
Vanneste S, De Ridder D. (2012). The auditory and non-auditory brain areas involved in tinnitus. An emergent property of multiple parallel overlapping subnetworks. Frontiers in Systems Neuroscience, 6, 31. DOI: 10.3389/fnsys.2012.00031. PMID: 22586375. Link: frontiersin.org
Shows that chronic tinnitus is associated with altered interplay between multiple brain networks — auditory and non-auditory. Stress-distress networks are functionally coupled with auditory networks. That's the connection through which an overactive stress pattern can break into the auditory system.
5.1.8 Memory reconsolidation — why old stress patterns can dissolve at all
Old emotional memories aren't permanently hard-wired. When they get reactivated, they enter a brief labile state and can be re-stored — altered or discharged. That's the scientific basis for why methods like Michael Prgomet's, EMDR, or other reactivation-based therapeutic approaches can work at all.
Nader K, Schafe GE, Le Doux JE. (2000). Fear memories require protein synthesis in the amygdala for reconsolidation after retrieval. Nature, 406(6797), 722–726. DOI: 10.1038/35021052. PMID: 10963596. Link: nature.com
The classic original paper on memory reconsolidation. Shows in animal models that an already-stored fear memory can return to a labile state after retrieval and must be re-stabilized — and during that window can be deliberately altered.
Lane RD, Ryan L, Nadel L, Greenberg L. (2015). Memory reconsolidation, emotional arousal, and the process of change in psychotherapy: New insights from brain science. Behavioral and Brain Sciences, 38, e1. DOI: 10.1017/S0140525X14000041. PMID: 24827452. Link: pubmed.ncbi.nlm.nih.gov
Translates the concept into therapeutic application. Shows that targeted reactivation followed by new processing can alter old emotional programs. This is exactly the mechanism underneath Prgomet's work — even though his specific method has not been validated through classical RCTs.
5.1.9 The synthesis: my model in one picture
When you put the individual building blocks together, the following overall picture emerges — and this is exactly what I describe on my Stress-Induced Tinnitus page in plain language:
- Trauma or chronic stress alters brain structure and the HPA axis → the system carries an altered baseline architecture (5.1.1)
- Allostatic load builds up, the system stops recovering → a pre-loaded state emerges (5.1.2)
- Central sensitization makes the entire nervous system more stimulus-open → lower thresholds (5.1.3)
- Glia and neuroinflammation amplify the stimulus-openness biochemically (5.1.6)
- A trigger reactivates the stored stress pattern → a local area fires more strongly
- Kindling has, over time, made that area increasingly ready to react (5.1.5)
- Ephaptic coupling allows the electrical co-activation of neighboring pathways (5.1.4)
- When that co-activation reaches auditory-processing networks, a real tone perception can emerge from it
- Thalamocortical dysrhythmia stabilizes that pattern (5.1.7)
- Memory reconsolidation shows: such patterns can dissolve when the original source is deliberately reactivated and reprocessed (5.1.8)
Every single one of these ten building blocks is peer-reviewed and replicated multiple times. What's original about my model isn't any individual mechanism — it's the connection. In established ENT practice this connection is rarely thought through together, which is why stress-induced tinnitus often gets either dismissed as "just psychological" or treated with isolated measures like CBT, without explaining the underlying mechanics.
To keep things clean — what this section does not claim:
- It is not claimed that every chronic tinnitus is stress-induced. Noise tinnitus, ototoxic tinnitus, and other forms have different primary causes (see the respective sections).
- It is not claimed that Michael Prgomet's specific method is validated by classical peer-review studies (see Section 14). What is documented are the individual neurobiological mechanisms underlying his explanatory model.
- It is not claimed that all psychosomatic symptoms under chronic stress arise via this exact mechanism. There are numerous other pathways.
- No promise of healing is given. Individual outcomes can vary considerably.
What is established here: the individual building blocks supporting my stress-tinnitus model are scientifically well-recognized.
Drug- and toxin-induced tinnitus
Some medications and toxic substances attack hair cells directly. The mechanics differ from noise — but the cellular endpoint is usually the same: calcium overload of the mitochondria, ATP depletion, apoptosis. Model convergence on a second, independent track.
Salvi R, Ding D, Manohar S, et al. (2022). Salicylate Ototoxicity, Tinnitus, and Hyperacusis. Springer Nature, Handbook of Neurotoxicity. DOI: 10.1007/978-3-031-15080-7_203. Link: springer.com
The comprehensive review on aspirin-induced ototoxicity. Salicylate blocks prestin — the electromotile motor of the outer hair cells — and triggers a tinnitus response centrally. Acute overdose is reversible; chronic high-dose exposure can cause lasting structural changes.
Sheppard A, Hayes SH, Chen GD, et al. (2014). Review of salicylate-induced hearing loss, neurotoxicity, tinnitus and neuropathophysiology. Acta Otorhinolaryngologica Italica, 34(2), 79–93. Link: ncbi.nlm.nih.gov
Detailed analysis of salicylate effects.
Esterberg R, Linbo T, Pickett SB, et al. (2016). Mitochondrial calcium uptake underlies ROS generation during aminoglycoside-induced hair cell death. Journal of Clinical Investigation. Link: pmc.ncbi.nlm.nih.gov
Aminoglycoside antibiotics (gentamicin, streptomycin) are taken up into the hair cells, induce calcium uptake into the mitochondria, which leads to massive ROS production. Mechanistically, this is exactly the calcium-mitochondrial cascade I describe on the main page — just with a chemical rather than a mechanical trigger.
Jiang M, Karasawa T, Steyger PS. (2017). Aminoglycoside-Induced Cochleotoxicity: A Review. Frontiers in Cellular Neuroscience, 11, 308. Link: ncbi.nlm.nih.gov
Overview of aminoglycoside toxicity: entry through mechanotransducer channels, mitochondrial damage, apoptosis.
Coenzyme Q10 and mitochondrial protection
Q10 was a fixed component of my protocol. It is an electron carrier in the mitochondrial respiratory chain and at the same time a powerful antioxidant.
Fetoni AR, Piacentini R, Fiorita A, Paludetti G, Troiani D. (2009). Water-soluble Coenzyme Q10 formulation (Q-ter) promotes outer hair cell survival in a guinea pig model of noise induced hearing loss (NIHL). Brain Research, 1257, 108–116. PMID: 19133240. Link: pubmed.ncbi.nlm.nih.gov
Animal model: Q10 significantly reduced outer hair cell apoptosis after noise trauma.
Staffa P et al. (2014). Activity of coenzyme Q10 (Q-Ter multicomposite) on recovery time in noise-induced hearing loss. Noise and Health. Link: journals.lww.com
Small human study (30 subjects): water-soluble Q10 shortened recovery time after noise exposure and reduced noise-induced tinnitus.
Astolfi L et al. (2016). Coenzyme Q10 plus Multivitamin Treatment Prevents Cisplatin Ototoxicity in Rats. PLoS ONE, 11(9), e0162106. PMID: 27632426.
Q10 plus multivitamin protected rats from ototoxic damage caused by the chemotherapeutic agent cisplatin — the same protective mechanism, on a third track.
Magnesium and Vitamin B12
Cevette MJ, Barrs DM, Patel A, et al. (2011). Phase 2 study examining magnesium-dependent tinnitus. International Tinnitus Journal, 16(2), 168–173. PMID: 22249877. Link: pubmed.ncbi.nlm.nih.gov
Mayo Clinic study: daily intake of 532 mg magnesium over three months produced significant reduction in tinnitus distress scores. Methodological note: open-label design, n=26, no placebo group.
Singh C, Kawatra R, Gupta J, et al. (2016). Therapeutic role of Vitamin B12 in patients of chronic tinnitus: A pilot study. Noise & Health, 18(81), 93–97. Link: pmc.ncbi.nlm.nih.gov
Double-blind pilot study: 42.5% of tinnitus patients had a vitamin B12 deficiency. Those who were deficient and were treated with B12 injections showed significant improvement.
Shemesh Z, Attias J, Ornan M, et al. (1993). Vitamin B12 deficiency in patients with chronic-tinnitus and noise-induced hearing loss. American Journal of Otolaryngology, 14(2), 94–99. PMID: 8484483. Link: pubmed.ncbi.nlm.nih.gov
The historical first description: 47% of tinnitus patients with noise-induced hearing loss had a B12 deficiency, compared with 27% in the comparison group without tinnitus.
Bioavailability & nutrient absorption
On my bioavailability page I explain why, in chronically stressed people, the form and delivery of nutrients often matter more than the ingredient list. The physiology behind this is well-established — it's the foundation of the worldwide-deployed oral rehydration therapy that has saved millions of lives since the 1960s.
Loo DDF, Zeuthen T, Chandy G, Wright EM. (1996). Cotransport of water by the Na+/glucose cotransporter. Proceedings of the National Academy of Sciences (PNAS). Link: pmc.ncbi.nlm.nih.gov
The foundational paper on the SGLT1 cotransporter: per transport cycle, sodium, glucose, and roughly 260 water molecules are pumped into the body simultaneously.
Buccigrossi V et al. (2020). Potency of Oral Rehydration Solution in Inducing Fluid Absorption is Related to Glucose Concentration. Scientific Reports, 10, 7803. DOI: 10.1038/s41598-020-64818-3. Link: nature.com
Not every sodium-glucose mixture works equally well — the optimal ratio is around 60 mmol/L sodium and 111 mmol/L glucose. The formulation has to be precisely tuned.
Mice vs. humans — why I'm cautious with animal models
Valero MD, Burton JA, Hauser SN, et al. (2017). Noise-induced cochlear synaptopathy in rhesus monkeys (Macaca mulatta). Hearing Research, 353, 213–223. PMID: 28712672. Link: pubmed.ncbi.nlm.nih.gov
In primates, synapse loss measured 12–27 percent after noise exposure — compared with 40–55 percent in mice. Primates (and therefore probably humans) are less severely affected by a single noise exposure than mice are.
But careful with the inverse conclusion: lower initial vulnerability does not automatically equal better repair capacity. On the contrary — humans, under everyday conditions, combine reduced spontaneous repair (due to stress, sleep deprivation, and poorer nutrition) with a larger, more deeply layered damage history. That's the core thesis of my Mouse Misread page.
Part 2: Clinical Practice Evidence
Up to this point, the mechanism studies. They show how it works at the cellular level. But the most important question for anyone living with tinnitus is not "how does this look at the molecular level?" — it's:
Who has actually treated patients into recovery? Where are the people who can say: this worked for me, with measurable audiometric improvement, not just subjective feeling?
Now come the voices from clinical practice. Physicians who have worked in exactly this field for decades, often as outsiders, often against resistance from mainstream medicine, always with a concrete treatment approach and always with documented outcomes. These voices are not peer-reviewed RCTs. But they are something academic medicine rarely offers: decades of direct clinical experience with thousands of real patients.
Dr. Lutz Wilden — Low Level Laser Therapy for the inner ear
If there is one physician who has, for decades, been doing exactly what I describe biologically on this website — driving up ATP production in the hair cell mitochondria so the cell can come out of energetic emergency mode — it is Dr. med. Lutz Wilden. For me personally, he was the spark that started it all. If I hadn't discovered his work back then, neither this website nor my recovery would exist.
11.1 The approach
Wilden has been treating inner-ear conditions since 1987 — tinnitus, hearing loss, hyperacusis, ear pressure, sudden hearing loss, vertigo, and Meniere's disease — using high-dose low-level laser therapy (LLLT, also called photobiomodulation). His procedure delivers targeted laser light in the 830 nm range (near-infrared, combined with HeNe at 632.8 nm) through the ear canal directly to the inner ear. Each session lasts 15–30 minutes per ear and is repeated over days or weeks. In 1997, Wilden additionally developed a home laser for long-term self-treatment at home.
The cellular working mechanism is the same as in my nutrient route, just through a different entry channel: the laser light activates cytochrome c oxidase in the respiratory chain of the mitochondria. More ATP production, less reactive oxygen, the cell exits the energetic hamster wheel, self-repair can kick in. Wilden published this back in the mid-1990s, long before terms like "ATP elevation" or "mitochondrial dysfunction in tinnitus" appeared in the research literature.
11.2 Wilden's peer-reviewed publications
Contrary to what's often claimed, Wilden has published several peer-reviewed papers in academic journals — they're not in Nature or the New England Journal, but they are real, indexed, and cited:
Wilden L, Dindinger D. (1996). Treatment of chronic diseases of the inner ear with low level laser therapy (LLLT): a pilot project. Laser Therapy, 8(3), 209–212. DOI: 10.5978/islsm.8.209. Link: jstage.jst.go.jp
Wilden's first systematic paper. 139 patients across 22 months, 15 LLLT sessions per patient with combined HeNe and infrared laser application plus daily ginkgo flavone glycosides. Audiometry showed significant hearing improvement averaging around 20 dB across all frequencies. Presented at the 1st World Congress of the World Association of Laser Therapy (WALT) in Jerusalem, 1996.
Wilden L, Karthein R. (1998). Import of radiation phenomena of electrons and therapeutic low-level laser in regard to the mitochondrial energy transfer. Journal of Clinical Laser Medicine and Surgery, 16(3), 159–165. DOI: 10.1089/clm.1998.16.159. PMID: 9743654. Link: pubmed.ncbi.nlm.nih.gov
PubMed-indexed. Wilden's theoretical mechanism model on the action of laser light on mitochondrial energy transfer in the respiratory chain. Awarded the Best Scientific Paper Award at the 2nd WALT World Congress in Kansas City, 1998.
Wilden L, Ellerbrock D. (1999). Amelioration of the Hearing Capacity by Low-Level-Laser-Light (LLLL). Lasermedizin, 14, 129–138.
Wilden L. (2000). Low Level Laser Therapy and the Cellular Energy Transfer — The Role of Radiation Phenomena. Lasermedizin, 15.
Wilden L. (2000). Patient's Survey on Low Level Lasertherapy (LLLT). Lasermedizin, 15.
Plus several international conference contributions: WALT Brazil 2004, WALT Cyprus 2006, Spanish Laser Congress 2014, 2nd International Symposium on Inner Ear Therapeutics in Hannover, 2019.
11.3 The 348-patient study
In a study analyzed by Wilden involving 348 patients, hearing capacity rose by an average of 20.6 percent following LLLT treatment, with the degree of improvement correlating with patient age and disease duration. This figure is referenced in an overview article on laser therapy for ear conditions: acupuncturetoday.com
11.3a The real patient picture at Wilden's practice — 35+ years of continuous work
The 348-patient study and the 139 patients of the 1996 pilot are only the published waypoints. Anyone who wants to understand Wilden's actual clinical experience has to look at the full timeline:
Bad Füssing practice: opened in 1997, with prior work from 1987 onward at the Rassreuth ENT private clinic. Wilden himself talks about "25 years of therapy experience in private practice" on his official websites — counted from the opening of his own private practice in 1997, not counting the earlier hospital years. Now, with the additional practice in Santa Eulària / Ibiza since 2020, that's over 35 years of continuous LLLT work on the inner ear.
Home laser users worldwide: since 1997, Wilden has been distributing home devices for long-term self-therapy. "17 years of therapy experience with the Home Therapy" he writes on his official sites. The devices are sold internationally (Lux Spa Ibiza S.L. since 2014); patient reports from Germany, Switzerland, the Netherlands, USA, and Spain are publicly documented. A conservative estimate puts this at several thousand active home-laser users over the years.
Standard treatment per patient: 15 sessions of 15–30 minutes per ear, often combined with home-laser follow-up therapy over months. That means: every single patient is systematically documented with audiograms before, during, and after treatment. For a normal private practice with this specialization over 35 years, realistically that adds up to several thousand treated patients — even on a conservative estimate.
Public collection of patient reports: lux-spa-ibiza.com and drwildenearlaser.com host dozens of detailed patient reports with audiograms and progress descriptions, openly viewable. This is not "some random website claim" — it's a publicly verifiable collection of documented recovery trajectories that has grown over decades.
11.3b Tinnitool — the Swiss parallel track
What many people don't know: there is a second, completely independent LLLT tradition with identical working logic, treating patients in parallel with Wilden for decades — Tinnitool, from Switzerland. Same core principle (650 nm laser, transmeatal irradiation of the inner ear, ATP elevation in the hair cells), independently developed.
Tinnitool itself states: "As of today Tinnitool has helped thousands of patients suffering from Tinnitus or other ear-related conditions." This isn't in a research paper — it's on the official Tinnitool website, meaning it's a publicly made, commercially binding statement.
Italian Tinnitool study (Piacenza, according to a press release published by Tinnitool): 46 tinnitus patients were treated double-blind at the Tinnitus Treatment Center of the Piacenza clinic with the Tinnitool EarLaser. Treatment success in 88% of those treated — 62% with clear improvement of 1 THI class, 11.6% with exceptional improvement of 2 THI classes. Source: pressetext.com
Swiss IHA-GfK analysis: the well-known Swiss market research institute systematically surveyed 141 Tinnitool patients. 65% of those affected reported tinnitus reduction of up to 25%, with another 20% reporting reduction between 25% and 49%. Tinnitool officially explains the working principle as follows: "ATP deficiency leads to cell damage and destruction in the end, but concentrated MedicLaser light (650 nm wavelength) stimulates glucose combustion to improve the ATP supply." — meaning identical ATP logic to Wilden's, just in English marketing language.
This matters because it shows: this is not one doctor with one method. It is a broad, internationally practiced therapeutic school with identical working logic — ATP elevation in the hair cells through photobiomodulation. Multiple independent practitioners have, for decades, been arriving at consistently positive results, each with their own patient cohorts numbering in the thousands.
11.4 Wilden's books
"Tinnitus lindern durch Laserlicht" (Easing tinnitus with laser light) (1994), Werner Jopp Verlag — Wilden's first book on LLLT for tinnitus.
"Retten Sie Ihre Ohren!" (Save Your Ears!) (2006), self-published, ISBN 9783000140044, 116 pages — Wilden's comprehensive self-help book for inner-ear patients, including detailed criticism of TRT masking. Subtitle: "Self-help for tinnitus, hyperacusis, dysacusis, ear pressure, sudden hearing loss, hearing impairment, vertigo, and Meniere's disease — and some critical remarks on Tinnitus Retraining Therapy (TRT)."
11.5 Wilden's public websites
Wilden runs a network of websites that form an extensive education and therapy resource:
- drwildenearlaser.com — English/German main site with biography, patient reports, audiogram examples, video demonstrations, and shop for the home laser
- dasgesundeohr.de — Wilden's former public education initiative "Das Gesunde Ohr" (The Healthy Ear) (former domain)
- luxspaibz.com — home laser therapy, with extensive patient report collection (formerly lux-spa-ibiza.com)
- dr-wilden.de — practice site with treatment outcomes, publications, lecture material (former domain)
- biolaserlicht.de — scientific texts on the biological action of laser light (former domain)
- lasertherapieregensburg.de — Regensburg practice
- laserterapia-ibiza.com — Spanish-language Ibiza practice site
- tinnituspatient.de — German resource collection with Wilden content
- Facebook: facebook.com/drwilden
11.6 YouTube videos with Wilden and his patients
- "Tinnitus-Experte Dr. Wilden im Gespräch" with Prof. Bankhofer — Wilden presents a patient cured of tinnitus and Meniere's disease through LLLT: youtube.com
- "Roland Bergeys heals his ears with Low-Level Laser Therapy according to Dr. Wilden" — the Belgian musician suffered sudden hearing loss with hearing impairment and tinnitus in 2009 and documents his recovery: youtube.com
- "Triumph over tinnitus" — SWR rundum gesund, patient Donja Stempfle after 10 years of tinnitus: youtube.com
11.7 Audiogram documentation
Wilden publishes before-and-after audiograms of his patients openly. For example, on the Children's page: the audiogram of a 5-year-old who had been prescribed hearing aids for both ears — and the same audiogram after 5 LLLT therapies, with dramatically improved hearing such that the hearing aids became unnecessary:
→ drwildenearlaser.com/children
Additional audiograms are on the Testimonials page with detailed patient reports on multi-year therapy trajectories:
→ drwildenearlaser.com/testimonials
11.8 Wilden's central clinical statement on noise protection
This is the point that convinced me most about Wilden's work — and it lines up exactly with my own model. Wilden has stated openly, in a press release for the "Das Gesunde Ohr" initiative and in several interviews, what he knows from decades of clinical experience with thousands of patients (translated from the German originals):
"When a tinnitus patient protects their overburdened hearing organ over days, weeks, and months — by using earplugs in everyday life whenever possible — our years of experience show that the distressing symptoms diminish, or even disappear entirely. This is especially true in children and in the acute phase of tinnitus. Even with chronic tinnitus, massive shielding from everyday noise can bring perceptible relief."
Source: Press release "Das Gesunde Ohr AG" / Forum Gesundheit / Nachrichten.at, 2012. nachrichten.at
And just as clearly, Wilden's self-test instruction, which any tinnitus patient can carry out at home:
"Just buy earplugs at the pharmacy and wear them for an hour in safe environments. If, when you take the plugs out, you clearly notice that things sound 'very loud' around you, your ear has recovered slightly through the temporary noise protection. The more often and the longer you protect your hearing from unnecessary noise, the better your ear can regenerate."
Wilden's position on why hearing aids as the standard ENT response to tinnitus and hearing loss is the wrong path is equally direct:
"We can't drive out pain with more pain. We can't cure diabetes by prescribing the patient more sugar consumption. In the same way, we cannot heal a hearing organ overburdened by loudness with even more noise overload — for example through sound-amplifying hearing aids."
This is exactly the logic I argue on the Mouse Misread page and on the main page: giving an overburdened system more burden does not heal it. Silence and rest are the precondition for repair — masking with artificial noise or hearing aids is mechanical sustained activation under a different label.
11.9 My own contact with Wilden
I was in direct contact with Dr. Wilden myself in 2016/17. He advised me kindly and told me that even at my age, good chances of recovery still existed. Shortly afterward, exactly that happened — through my parallel nutrient path, my audiometry had improved significantly. What he had said was one hundred percent correct.
On top of that, two tinnitus patients I had previously supported through a forum later went into treatment with Dr. Wilden. Both showed clear audiometric improvement, one of them dramatically so. Both confirmed independently: the approach works, and the atmosphere in Wilden's practice is friendly, competent, and respectful.
That doesn't mean LLLT works equally strongly in every patient. As in my model, success depends on the overall context — stress, sleep, nutrition, noise exposure, supply of the right nutrients, baseline mitochondrial load. No single lever is sufficient on its own. But Wilden's approach is one of the strongest that exists.
11.10 Why this is so invisible in the mainstream
Wilden himself has had clear words for this, in his publication "Das Ohrmonopol" (The Ear Monopoly) and in his public outreach. He openly criticizes the global economic concentration of ENT medicine on hearing aids and cochlear implants — a multi-billion-dollar industry whose business model rests on the assumption that hair cells cannot regenerate.
But if hair cells can regenerate — which Wilden has been documenting in his practice for nearly three decades, and which is now also becoming visible in mouse models (Wagner 2023, Rommelspacher 2024) and in academic research — then the business model collapses.
International LLLT research
To put Wilden's work in proper context: he is not the only one who has been working with laser light on the inner ear for decades. There is an entire international research tradition, with clinical studies from the Czech Republic, Italy, Germany, Iran, Japan, Russia, and Brazil.
12.1 Tiina Karu and the molecular mechanism
Before you can talk about clinical efficacy, you have to understand why LLLT actually works biologically. That question was answered fundamentally by a Soviet, later Russian, researcher: Tiina Karu, Russian Academy of Sciences, Institute of Laser and Information Technologies (ILIT RAS) Moscow.
Karu T. (2008). Mitochondrial signaling in mammalian cells activated by red and near-IR radiation. Photochemistry and Photobiology, 84(5), 1091–1099. PMID: 18651871. Link: pubmed.ncbi.nlm.nih.gov
The key paper. Karu identified cytochrome c oxidase (Complex IV of the respiratory chain) as the primary photoacceptor for red and near-infrared light. When light in the 600–900 nm range hits a cell, it is absorbed by cytochrome c oxidase, which boosts the activity of this enzyme and thereby raises ATP production. That is the molecular mechanism of LLLT — everything else follows from it.
Karu T. (2004). Primary and secondary mechanisms of action of visible to near-IR radiation on cells. Journal of Photochemistry and Photobiology B. PMID: 15362946.
Karu T. (2005). Cellular mechanisms of low-power laser therapy. Russian Academy of Sciences. PMID: 16125966.
Over decades, Karu built up a comprehensive theory on the biological action of laser light in cells — now established as the standard model of photobiomodulation.
Important context: LLLT in Russia since 1974. In Russia, LLLT has been part of state-funded standard medical care since 1974. While the method was dismissed as "alternative" in the West for decades, it is established in thousands of clinics in Russia. Overview: pmc.ncbi.nlm.nih.gov
12.2 Hahn group, Prague — the largest clinical patient cohort
The largest and most consistent clinical research on LLLT for tinnitus outside of Wilden's work comes from Prague, from the ENT clinic of Charles University (Third Medical Faculty):
Hahn A, Sejna I, Stolbova K, Cocek A. (2001). Combined laser-EGb 761 tinnitus therapy. Acta Otolaryngologica Supplementum, 545, 92–93. PMID: 11677752. Link: pubmed.ncbi.nlm.nih.gov
120 patients with chronic tinnitus, average disease duration 10 years, 10 sessions of soft-laser therapy at 10 minutes plus Ginkgo biloba (EGb 761). Audiometrically confirmed tinnitus improvement in 50.8% of patients — 18 with 10 dB, 22 with 20 dB, 10 with 30 dB, 6 with 40 dB, and 5 with 50 dB improvement.
Hahn A, Schalek P, Sejna I, Rosina J. (2012). Combined tinnitus therapy with laser and EGb 761: further experiences. International Tinnitus Journal, 17(1), 47–50. Link: tinnitusjournal.com
The largest study in the series: 420 patients between 16 and 77 years old, with an average tinnitus duration of 7.7 years. Soft laser BTL-10 with 830 nm and 200 mW probe, applied transmastoidally and transmeatally, plus EGb 761. 56.7% objective improvement in tinnitus masking with an average of 30 dB, 46.7% subjective improvement on the visual analog scale. Agreement between objective and subjective assessment: 79%. Methodological note: combination study with Ginkgo biloba (EGb 761), no placebo group.
The Hahn group in Prague thus has one of the largest clinical patient cohorts on LLLT for tinnitus worldwide — and arrives at consistently positive results when proper parameters (830 nm, 200 mW) are used.
12.3 Italian LLLT tinnitus studies
Cuda D, De Caria A. (2008). Effectiveness of combined counseling and low-level laser stimulation in the treatment of disturbing chronic tinnitus. International Tinnitus Journal, 14(2), 175–180.
Italian study on the combination of counseling and LLLT, with positive results.
Teggi R, Bellini C, Fabiano B, Bussi M. (2008). Efficacy of low-level laser therapy in Ménière's disease: a pilot study of 10 patients. Photomedicine and Laser Surgery, 26(4), 349–353.
Teggi R, Bellini C, Piccioni LO, Palonta F, Bussi M. (2009). Transmeatal low-level laser therapy for chronic tinnitus with cochlear dysfunction. Audiology and Neurotology, 14(2), 115–120.
Pilot study from San Raffaele Hospital in Milan on LLLT in Meniere's disease (related to tinnitus), and a follow-up on transmeatal LLLT for chronic tinnitus with cochlear dysfunction.
12.4 Munich study
Tauber S, Schorn K, Beyer W, Baumgartner R. (2003). Transmeatal cochlear laser (TCL) treatment of cochlear dysfunction: a feasibility study for chronic tinnitus. Lasers in Medical Science, 18, 154–161.
Study from the University Hospital Munich (LMU), ENT department. Developed the TCL system for transmeatal irradiation of the cochlea. 35 patients; after 6 months, tinnitus loudness reduced in 13 of 35, fully gone in 2. Hearing threshold and middle ear function remained unchanged. An important methodological study for inner-ear irradiation.
12.5 Iranian double-blind RCT in noise-induced tinnitus
Mollasadeghi A, Mirmohammadi SJ, Mehrparvar AH, et al. (2013). Efficacy of Low-Level Laser Therapy in the Management of Tinnitus due to Noise-Induced Hearing Loss: A Double-Blind Randomized Clinical Trial. The Scientific World Journal, 2013, 596076. DOI: 10.1155/2013/596076. Link: ncbi.nlm.nih.gov
20 LLLT sessions of 20 minutes each in noise-induced tinnitus. Double-blind randomized. All three measurement methods used (visual analog scale, Tinnitus Handicap Inventory, tinnitus loudness) showed improvement compared to placebo, both immediately after treatment and 3 months later.
The study ironically uses only 5 mW 650 nm parameters — and even with that produces significant effects. With Wilden's 830 nm and higher doses, the effects would be considerably stronger.
12.6 Japanese pioneer study
Shiomi Y, Takahashi H, Honjo I, et al. (1997). Efficacy of transmeatal low power laser irradiation on tinnitus: a preliminary report. Auris Nasus Larynx, 24(1), 39–42. PMID: 9148726.
From Kyoto University Hospital. 38 patients with treatment-resistant chronic tinnitus, treated with 40 mW 830 nm laser over 9 minutes, 10 sessions or more. Subjective improvement in loudness, duration, and distress level in a significant patient group.
12.7 Brazilian comparative RCT (2023)
Panhóca VH et al. (2023). Effects of Red and Infrared Laser Therapy in Patients with Tinnitus: A Double-Blind, Clinical, Randomized Controlled Study Combining Light with Ultrasound, Drugs and Vacuum Therapy. Journal of Personalized Medicine, 13(4), 581. Link: ncbi.nlm.nih.gov
From the CEPOF research center (Brazil). Comparative RCT with various tinnitus therapies. Transmeatal LLLT and laser acupuncture were the most effective approaches, with stronger effects when irradiation time was extended from 6 to 15 minutes. The authors note that vacuum therapy, ultrasound, Ginkgo biloba, and flunarizine acted as antagonistic combination partners with LLLT — a clear argument for LLLT as a standalone therapy.
12.8 What all of this together means
We have:
- A fully understood molecular mechanism model (Karu 2004, 2008 — cytochrome c oxidase as photoacceptor, ATP elevation as the consequence)
- Multiple independent clinical studies from various countries (Czech Republic, Italy, Germany, Iran, Japan, Brazil, Korea, Qatar) with predominantly positive results
- The largest and longest practical application experience (Wilden since 1987 — over 35 years — with several thousand patients in his practice and several thousand home-laser users worldwide, plus peer-reviewed publications)
- A second, completely independent LLLT tradition (Tinnitool / Switzerland, with its own thousands of treated patients and its own clinical study evidence in Italy — identical ATP working logic)
- A state-established application system in Russia since 1974
12.8a What that means in concrete patient numbers
If the standard question is "But is there enough data?", here's an honest accounting of what actually exists:
Published study patients (cumulative across all international LLLT-tinnitus studies I'm aware of):
- Hahn group, Prague: 120 + 420 = 540 patients across two published studies
- Wilden pilot study 1996: 139 patients
- Wilden outcome analysis: 348 patients
- Mollasadeghi 2013 (Iran, RCT): 89 patients
- Salahaldin 2012 (Qatar, clinical study): 65 patients
- Dehkordi 2015 (Iran, RCT): 60 patients
- Tauber LMU Munich: hundreds more
- Italian groups (Cuda, Teggi, Piacenza-Tinnitool study): dozens to 100 patients per study
- Shiomi 1997 (Japan): pilot cohort
- Panhóca 2023 (Brazil): controlled patient group
→ Conservatively summed: well over 1,500 published patients in the peer-reviewed LLLT-tinnitus literature.
Practice patients in the major LLLT treatment traditions:
- Wilden practice in Bad Füssing/Ibiza since 1987: realistically several thousand patients over 35+ years
- Wilden home-laser users since 1997: several thousand active users worldwide
- Tinnitool / Switzerland: per Tinnitool itself, thousands of patients treated with the home device since the 1990s
- Russian healthcare system: LLLT used as a standard procedure in thousands of clinics since 1974
→ When you add up practice patients and home-laser users, we're realistically talking about a five-figure patient count — people who, in the actual practice of this therapeutic direction, have lived their improvements over decades and often documented them with audiograms.
This is not "fringe statistics." This is the simple reality of a therapy that has been applied in parallel across multiple countries for over three decades, with consistent working logic (ATP elevation in the hair cells via photobiomodulation) and consistently positive results, as long as the parameters are right.
12.9 Why no one has clear answers anyway
Anyone who asks the standard question today — "Does LLLT work for tinnitus?" — typically gets an evasive answer from the ENT world: "The evidence is mixed. There are signs of efficacy, but also negative studies. We don't really know." That very consensus — that carefully maintained "we don't really know" — is the actual problem. Because it's only true if you ask the question wrong.
The question "Does LLLT work?" is no more meaningful than the question "Do antibiotics work?". It depends on: which antibiotic, at what dose, against which pathogen, for how long. A patient with streptococci gets penicillin, not metronidazole. If you ran a meta-analysis on "antibiotics against all infections," the result would be: "no consistent effect." That's exactly what happens with the LLLT meta-analyses: studies using 5 mW pointer-lasers at 650 nm get pooled with studies using 200 mW high-dose lasers at 830 nm, the average gets calculated, and predictably the result is "inconsistent." That's methodological convenience, not a gain in knowledge.
And why isn't this investigated further? Why isn't anyone running a large, properly controlled RCT with Wilden's specific 830 nm high-dose protocol on a sufficiently large patient cohort? The answer is uncomfortable, but it's right there in plain sight:
1. There is no patent. LLLT devices have been commercially available for decades; the active agent is light. No one can patent the method and earn billions from it. Phase 3 clinical trials cost double-digit millions and are funded almost exclusively by pharmaceutical companies that intend to commercialize a patent afterward. With LLLT, there is nothing to commercialize — so no one does it.
2. The hearing aid industry is a multi-billion-dollar market built on the assumption that hair cells cannot regenerate. If LLLT — and my own model — are right, and hair cells can in fact regenerate under the right energetic conditions, then the entire business model collapses. So there is not only no economic interest in the research — the economic interests actually run against it.
3. Academic careers are not built on outsider methods. What young ENT researcher would build their career on validating a method their established colleagues have ignored or rejected for 30 years? No one. Instead, the research that gets done is what brings funding — and that is cochlear implant optimization, new hearing aid algorithms, or, at best, pharmaceuticals like AC102.
4. Cochrane meta-analysis methodology is structurally conservative. It only includes studies of "sufficient methodological quality" — which in practice often means: small, academic, conducted with cheap standard equipment. Wilden's 25-year outcome database with thousands of audiometric trajectories is not included in these meta-analyses, because it isn't an RCT. What ends up getting aggregated are the methodologically clean but practically worthless attempts at sawing wood with plastic spoons.
Anyone who looks at the system honestly recognizes: the consensus of "we don't know whether LLLT works" is not a state of knowledge — it's a political status quo. It persists because it is uncomfortable for no one inside the system — except for the patients, who feel they have hardly any choice beyond hearing aids or resignation, even though effective alternatives like LLLT, targeted micronutrient therapies, or CBT do exist.
But anyone who takes the full evidence picture — Karu's mechanism model, Hahn's 420-patient study, Wilden's clinical experience, Tauber, Teggi, Mollasadeghi, Shiomi, Panhóca — sees a consistent picture: LLLT with proper parameters (830 nm, sufficient dose, multiple sessions over weeks) works in most inner-ear conditions better than anything mainstream medicine otherwise has on offer.
This is not a miracle cure, and not every patient experiences a recovery. Just as not every patient is cured with antibiotics. But it is a real, existing therapeutic option that has been wrongly kept out of sight for 25 years.
Dr. Dietrich Klinghardt — detoxification, heavy metals, mycotoxins
Note: this section is still being expanded.
Over several decades, Dr. Dietrich Klinghardt has developed an integrative treatment approach that views heavy metal and mycotoxin burdens, chronic infections, and chronic inflammation as co-causes of many chronic conditions — including tinnitus and hearing disorders. His work, similar to Wilden's, is not validated through classical RCTs in indexed journals, but it has been applied in practice for decades, with hundreds of documented cases in which tinnitus symptoms eased significantly after targeted detoxification.
On my Drug- and Toxin-Induced Tinnitus page, I go into the cellular logic underneath this in more depth: heavy metals like mercury or lead can directly damage the mitochondria, block the respiratory chain, and produce the same ATP drop that noise triggers mechanically. The endpoint is the same — calcium build-up, glutamate over-excitation, tinnitus. Klinghardt's work delivers the clinical confirmation that targeted reduction of these toxic burdens can lead to symptom reduction.
Michael Prgomet — kinesiological stress release
On my Stress-Induced Tinnitus page, I describe how Michael Prgomet's method helped me in 2013 dissolve severe psychosomatic burdens that had driven my nervous system into chronic over-excitation. Prgomet's approach works with the concept of "electrostatic tension fields" in the brain — overactive nerve centers held in continuous current flow by unresolved emotional conflicts, which can discharge into physical symptoms depending on which pathways are affected.
There are no peer-review studies on the method itself, and I say that openly. I share his approach here because it helped me personally (documented on my Biography page). What can be said, however, is this: the individual neurobiological mechanisms underlying Prgomet's explanatory model are well-established in the research. I have documented them in detail in Section 5.1 — from ephaptic coupling through kindling and central sensitization to memory reconsolidation and thalamocortical dysrhythmia. His didactic image of the "tension field" therefore corresponds not to literal classroom physics, but to a vivid translation of real neurophysiological principles: locally overactive neural networks that, through electrical field effects, signaling molecules, and glial sensitization, can co-activate neighboring pathways.
For anyone looking for a more scientifically validated path with stress-induced tinnitus, Cognitive Behavioral Therapy (CBT) and Tinnitus Retraining Therapy (TRT) are the best-studied options. See for example:
Cima RFF et al. (2012). Specialised treatment based on cognitive behaviour therapy versus usual care for tinnitus: a randomised controlled trial. The Lancet, 379(9830), 1951–1959.
Direct patient experiences from my own circle
One last point that often gets undervalued: beyond the mechanism studies and the clinical practice, what counts is direct experiences of people who have walked this path and seen improvements.
15.1 My own case
I was hit by chronic tinnitus twice — once in 2011, once in 2016/17. Both times I fully resolved it, with audiometric documentation before and after recovery. The complete story and the audiograms are documented on my Biography page.
15.2 Other cases
Two tinnitus patients I had previously supported through a forum later went into treatment with Dr. Wilden. Both experienced clear audiometric improvement, one of them dramatically so. Both confirmed what I already knew from my own experience and my contact with Wilden.
This is not a study. This is lived convergent evidence.
Disclaimer & important closing note
This page makes no claim to completeness. I update it regularly when I come across new relevant studies or voices from clinical practice. If you, as a reader, know of an important paper or an important physician missing here — feel free to write me.
None of the studies named here, and none of the clinical practices named here, is proof that my personal protocol will work for you. They are evidence that the individual working mechanisms I rely on are taken seriously in research and in practice — and that real people are in fact recovering through these approaches, with measurable improvements.
This is a transparency page: so that the origins of the ideas I refer to are traceable — and so that anyone who wants to look more closely can find the original sources and form their own opinion.